


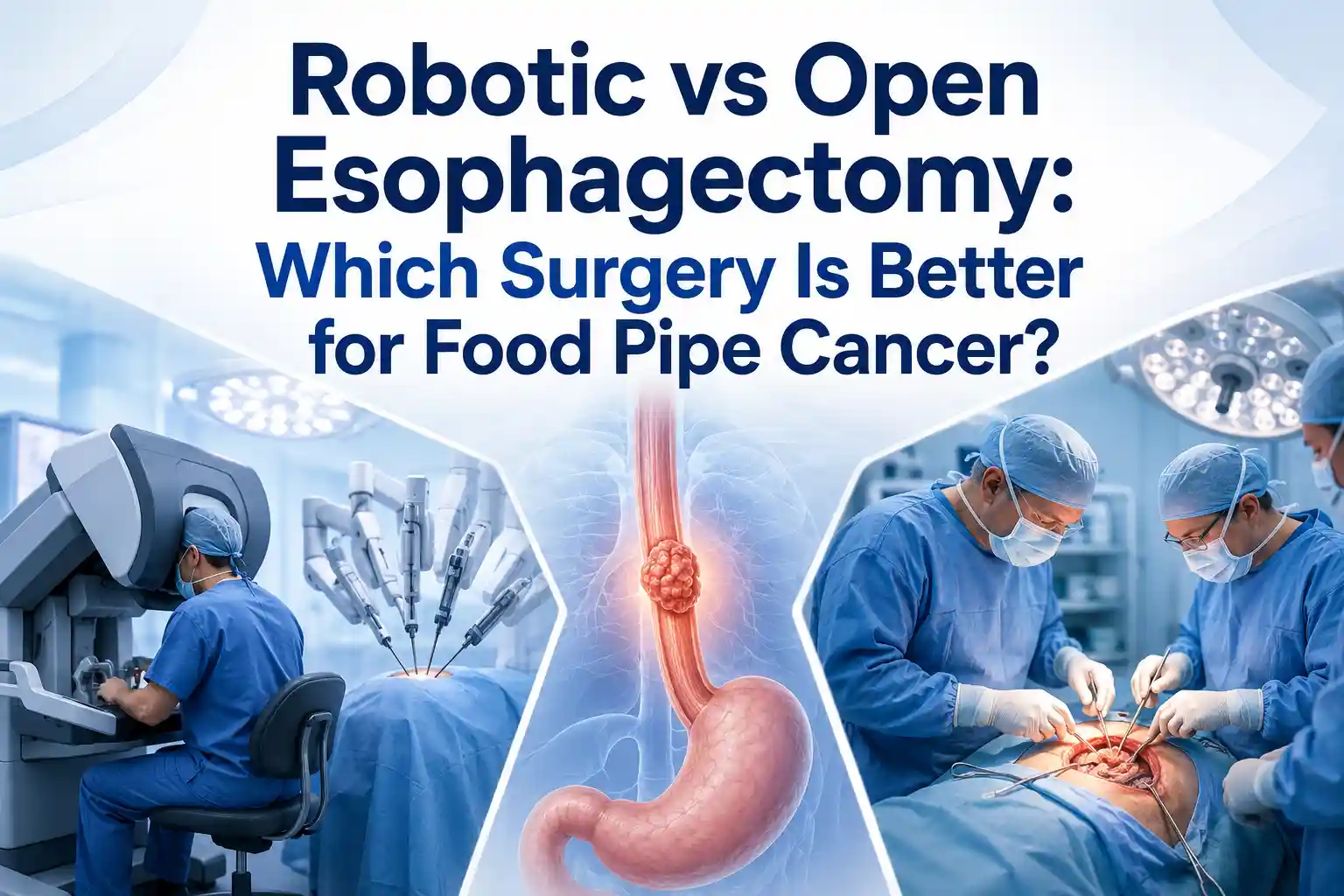
When someone is diagnosed with food pipe cancer, one of the biggest decisions is choosing the right surgery. Many patients and families search for robotic vs open esophagectomy because they want to know which approach is safer, less painful, more effective, and better for recovery.
Esophagectomy is the surgery used to remove part or most of the esophagus, also called the food pipe. The remaining healthy part is then connected to the stomach or, in some cases, another part of the intestine so that the patient can swallow again. The National Cancer Institute explains that surgery is a common treatment for esophageal cancer, and lymph nodes near the esophagus may also be removed and checked for cancer cells.
The main question is not simply, “Which surgery is latest?” The better question is, “Which surgery is safest and most suitable for this patient’s cancer stage, body condition, and recovery needs?”
For patients looking for esophageal cancer surgery in Gurgaon, understanding the difference between robotic surgery and open surgery can help them ask better questions before treatment.
In open esophagectomy, the surgeon operates through one or more large incisions in the chest, abdomen, or neck. The American Cancer Society explains that open esophagectomy may involve large cuts in the neck, chest, abdomen, or a combination of these areas.
In robotic esophagectomy, also called robot-assisted minimally invasive esophagectomy or RAMIE, the surgeon operates through small keyhole incisions using robotic instruments. The surgeon controls the robotic arms from a console. The robot does not operate on its own.
The American Cancer Society states that robotic-assisted laparoscopic surgery is one type of minimally invasive esophagectomy, where the surgeon sits at a control panel and moves precise robotic arms with surgical instruments.
Both surgeries aim to do the same cancer operation:
The difference is mainly in how the surgeon reaches the esophagus.
During esophagectomy, the surgeon removes the diseased part of the food pipe. Depending on where the tumor is, part of the stomach may also be removed. The stomach is often pulled up and connected to the remaining esophagus. In some cases, a part of the intestine may be used for reconstruction.
Mayo Clinic explains that esophagectomy may remove part of the esophagus, part of the top of the stomach, and nearby lymph nodes, depending on the cancer stage and tumor location.
This is a major operation. It needs careful planning, proper staging, lung and heart fitness assessment, nutrition support, and an experienced surgical team.
Open esophagectomy is the traditional method. It gives the surgeon direct access to the chest and abdomen through larger incisions. In some patients, this wide access can be useful, especially when the tumor is complex.
Open surgery may be done through different approaches, such as:
Open surgery can be effective for cancer removal, but because it involves larger cuts, it may lead to more pain, more trauma to the chest wall, longer recovery, and higher risk of breathing-related problems in some patients.
The American Cancer Society notes that esophagectomy is not a simple operation and should ideally be done at a center with significant experience in treating esophageal cancer and performing these surgeries.
Robotic esophagectomy is a more advanced form of minimally invasive esophagectomy. The surgeon makes small incisions and uses robotic arms with tiny instruments. A high-definition 3D camera gives a magnified view of the surgical area.
Mayo Clinic explains that robotic surgery allows doctors to perform complex procedures with more precision, flexibility, and control than traditional methods. It also provides a magnified, high-definition 3D view of the surgical site.
For esophageal cancer, this can be helpful because the food pipe is located close to important structures such as the lungs, heart, airway, major blood vessels, lymph nodes, and nerves.
At Chest Surgery India, robotic thoracic surgery is used for selected thoracic conditions, including robotic-assisted esophagectomy for esophageal cancer. The website also mentions the use of ICG fluorescence imaging in esophageal surgery to check blood supply to the reconstructed food pipe in real time.
One of the most visible differences between open surgery vs robotic surgery for esophageal cancer is incision size.
Open surgery usually needs one or more large incisions. In chest surgery, this may also involve spreading the ribs, depending on the approach. This can cause more chest wall pain and may make coughing or deep breathing difficult after surgery.
Robotic surgery uses several small cuts. Smaller cuts generally mean less trauma to the body. Mayo Clinic notes that minimally invasive esophagectomy, including robot-assisted techniques in suitable patients, may be performed through several small cuts and can result in reduced pain and faster recovery compared with conventional surgery.
This is one reason why many patients ask about robotic food pipe cancer surgery when they are fit for a minimally invasive approach.
Pain after esophagectomy is expected because it is a major cancer surgery. However, the level of pain may differ based on the surgical approach.
Open surgery can cause more pain because of larger incisions and greater chest wall trauma. Robotic surgery may reduce pain because it avoids large cuts in selected patients. This can help patients breathe better, cough better, walk earlier, and participate more comfortably in recovery exercises.
That said, robotic surgery is not pain-free. Patients still need proper pain medicines, breathing exercises, nutrition support, and follow-up care.
Blood loss can vary from patient to patient. Tumor size, previous chemotherapy or radiation, scarring, patient health, and surgical complexity all matter.
Research suggests that robotic esophagectomy may reduce blood loss compared with open surgery. A JAMA Network Open systematic review and meta-analysis found that, compared with open esophagectomy, robot-assisted minimally invasive esophagectomy was associated with decreased estimated blood loss, fewer pulmonary complications, and fewer total complications, although operative time was longer.
This does not mean robotic surgery is automatically safer for everyone. It means that in properly selected patients, robotic surgery may offer short-term recovery benefits.
A common fear among patients is: “If the cuts are smaller, will the cancer removal be weaker?”
The answer is no, not when the surgery is done properly by an experienced surgeon. The cancer goals remain the same in both robotic and open esophagectomy. The surgeon must remove the tumor with safe margins and remove nearby lymph nodes for staging.
The American Cancer Society states that nearby lymph nodes are removed during either type of esophagectomy and checked in the lab for cancer cells. It also notes that at least 15 lymph nodes are typically removed during surgery.
Robotic surgery may help in lymph node dissection because of magnified 3D vision and precise instruments. The JAMA review found that lymph node harvest was not worse with robotic surgery compared with video-assisted minimally invasive esophagectomy, and evidence suggested larger lymph node harvest with robotic surgery compared with open surgery in some comparisons.
The key point is clear: the choice of surgeon and hospital experience matters as much as the choice of technique.
Lung complications are one of the biggest concerns after esophageal cancer surgery. These may include pneumonia, fluid around the lungs, breathing difficulty, or longer ICU and hospital stay.
The American Cancer Society lists lung complications, including pneumonia, as common risks after esophagus surgery.
This is where minimally invasive and robotic surgery may offer an important advantage. In the JAMA Network Open meta-analysis of 21 studies involving 9,355 patients, robotic esophagectomy was associated with fewer pulmonary complications than video-assisted minimally invasive esophagectomy and open esophagectomy.
For patients with a history of smoking, COPD, asthma, weak lungs, or previous chest illness, this discussion becomes even more important. However, lung fitness must be evaluated before surgery through clinical examination and tests such as pulmonary function tests.
Recovery after esophagectomy depends on many factors:
Robotic surgery may allow faster recovery in selected patients because of smaller incisions, less pain, and earlier mobility. Mayo Clinic notes that minimally invasive surgery can support shorter hospital stay and quicker recovery in general robotic procedures, while also making it clear that robotic surgery is not suitable for everyone.
After esophagectomy, patients usually need small frequent meals because the stomach size and position may change. Mayo Clinic notes that after esophagectomy, some patients may need tube feeding at first, and once regular diet resumes, smaller and more frequent meals may be needed.
In most hospitals, robotic esophagectomy may cost more than open surgery. The difference may be due to robotic system charges, disposable instruments, operating room time, hospital stay, ICU needs, and case complexity.
However, cost should not be judged only by the surgery package. Patients should also consider:
In some patients, faster recovery and fewer complications may reduce overall burden. In others, open surgery may be the more practical or safer option. The right decision should be based on medical suitability, not only cost.
Robotic surgery may be preferred when:
For patients searching for robotic thoracic surgery in Gurgaon, it is important to ask whether robotic surgery is truly suitable for their specific case, not just whether the technology is available.
Open surgery still has an important role. It may be safer or more suitable when:
A good surgeon should know when to use robotic surgery and when not to use it. Chest Surgery India’s robotic thoracic surgery page also explains that robotic surgery is not right for every patient and that open surgery may remain safest for very large tumors invading the heart or great vessels, severe scarring, or emergency situations.
Many patients also search for MIE vs open esophagectomy. MIE means minimally invasive esophagectomy. It includes laparoscopic, thoracoscopic, and robotic-assisted approaches.
In simple terms:
Chest Surgery India already has a detailed patient guide on MIE vs open esophagectomy, which explains how minimally invasive approaches may reduce tissue trauma, pain, blood loss, lung complications, and hospital stay while maintaining cancer surgery goals.
There is no one answer for every patient.
For many suitable patients, robotic esophagectomy may offer advantages such as:
For some patients, open surgery may be better because it gives wider access and may be safer in complex cancer cases.
The American Cancer Society states that minimally invasive approaches may allow patients to leave the hospital sooner, have less pain, and recover faster, but they may not be best for everyone depending on where the cancer is and how difficult it is to remove. It also notes that surgeon skill and experience are often the most important factors.
So, the best surgery is the one that gives the safest cancer removal with the lowest practical risk for that patient.
Before deciding between robotic and open esophagectomy, ask:
A confident and experienced surgeon should answer these questions clearly.
Esophagectomy is a complex surgery, whether it is open, minimally invasive, or robotic. The technology matters, but the surgeon’s judgment matters more.
Dr. Parveen Yadav is listed as having 18+ years of experience in oncology and 12+ years in thoracic surgery, with more than 5,700 major thoracic procedures, including over 1,000 surgeries for esophageal cancer and other esophageal diseases.
Chest Surgery India also notes that Dr. Yadav specializes in minimally invasive and robotic lung and esophageal surgeries at Artemis Hospital, Gurgaon.
For patients comparing food pipe cancer surgery options in Gurgaon, Delhi NCR, or India, these experience signals are important. They help patients judge whether the treatment plan is based on real surgical expertise, not just availability of technology.
The comparison of robotic vs open esophagectomy is not about choosing the newest surgery blindly. It is about choosing the safest and most effective approach for the patient.
Robotic esophagectomy may offer smaller cuts, less pain, reduced blood loss, fewer pulmonary complications, and smoother early recovery in selected patients. Open esophagectomy may still be better for complex tumors, severe scarring, emergency situations, or cases where wider access is needed.
The right decision should be made after complete staging, PET CT or CT review, biopsy confirmation, lung and heart fitness evaluation, nutrition assessment, and discussion with an experienced thoracic cancer surgeon.
If you or your loved one has been advised surgery for food pipe cancer, consult Dr. Parveen Yadav at Chest Surgery India, Artemis Hospital, Gurgaon, for a detailed evaluation. You can learn more about esophageal cancer surgery in Gurgaon and discuss whether robotic, minimally invasive, or open esophagectomy is the right approach for your case.
Robotic esophagectomy uses small keyhole incisions and surgeon-controlled robotic instruments. Open esophagectomy uses one or more large incisions in the chest, abdomen, or neck. Both aim to remove the cancer and reconstruct the food passage.
Robotic esophagectomy may offer benefits such as smaller incisions, less pain, less blood loss, fewer lung complications, and faster early recovery in selected patients. Open surgery may still be safer for large or complex tumors.
Cancer removal depends mainly on proper staging, surgical planning, clear margins, lymph node removal, and surgeon experience. In suitable patients, robotic surgery can achieve cancer surgery goals without compromising treatment.
Robotic surgery is still major surgery, so some pain is expected. However, because it uses smaller incisions, pain may be less than open surgery in many selected patients.
Open esophagectomy may be recommended for very large tumors, cancers involving nearby vital structures, severe scarring from previous surgery, emergency situations, or cases where robotic surgery may not be safe.
MIE means minimally invasive esophagectomy. It uses small incisions instead of large cuts. Robotic esophagectomy is an advanced form of MIE. Open esophagectomy uses larger incisions.
In suitable patients, robotic and minimally invasive surgery may support shorter hospital stay and faster recovery because of smaller incisions and less trauma. However, hospital stay depends on healing, nutrition, lung function, and complications.
You can consult Dr. Parveen Yadav at Chest Surgery India, Artemis Hospital, Gurgaon, for evaluation of robotic, minimally invasive, and open surgery options for esophageal cancer.
References Used
https://www.cancer.gov/types/esophageal/patient/esophageal-treatment-pdq
https://www.cancer.org/cancer/types/esophagus-cancer/treating/surgery.html
https://www.mayoclinic.org/tests-procedures/esophagectomy/about/pac-20385084
https://www.mayoclinic.org/tests-procedures/robotic-surgery/about/pac-20394974
https://jamanetwork.com/journals/jamanetworkopen/fullarticle/2785662
18+ Yrs Exp | 5,700+ Thoracic & Robotic Cancer Surgeries
Dr. Parveen Yadav is a Director and Senior Consultant in Thoracic and Surgical Oncology, specializing in minimally invasive and robotic lung and esophageal surgeries, with advanced training from AIIMS and Tata Memorial Hospital.
View Full Profile
Understand the esophageal cancer surgery recovery timeline from the first week to 3 months, including diet, pain, walking, breathing exercises, follow-up, and warning signs.

Learn when to take a second opinion for esophageal cancer in India, what reports to share, and why expert review matters before surgery, chemotherapy, or radiation.
Know the important tests before esophageal cancer surgery, including endoscopy biopsy, PET CT, EUS, blood tests, lung fitness, and cardiac evaluation.
Copyright 2026 © Dr .Parveen Yadav all rights reserved.
Proudly Scaled by Public Media Solution!