



Sandesh was 54 years old when he got the news no one wants to hear. A shadow on his lung scan. A biopsy. Stage 2 lung cancer. After weeks of fear and sleepless nights, he finally made it through surgery at a hospital in Delhi. The tumour was removed. His family wept in the waiting room. The surgeon walked out and said those words every patient prays for: the operation went well.
But three days after coming home, Sandesh could not sleep. He was lying still in bed, and yet every breath felt like someone pressing a fist between his ribs. A sharp, aching pain had crept into his right shoulder, and his mind went straight to the worst: had something happened to his heart? Was the cancer still there?
He had not been warned about this. Nobody had explained what recovery from thoracic surgery actually feels like. And Sandesh is not alone. This is one of the most common gaps in patient care after chest surgery: people get tremendous support during the operation itself, but very little guidance on what comes next.
That is exactly what I want to fix with this guide.
Pain after thoracic surgery is normal, expected, and most importantly, manageable. But managing it well requires knowledge that most discharge sheets never provide. Whether you or someone you love is recovering from lung cancer surgery, esophageal surgery, or another chest procedure, this guide walks through what is really happening in your body, what tools you have at your disposal, and what the warning signs are that should never be ignored.
What Is Thoracic Surgery Recovery? The recovery period after thoracic surgery refers to the weeks following a chest procedure during which the body heals incisions, rebuilds lung function, and manages pain while preventing complications like pneumonia or blood clots. |
50%+ of thoracotomy patients experience some chronic pain after surgery (BJA Education Journal) | 57% develop neuropathic pain at 3 months post-op (Journal of Pain meta-analysis) | 50% reduction in chronic pain risk when epidural analgesia is used aggressively after surgery (UVA ERAS Study) |
Here is the surprising truth about thoracic surgery pain: it is considered one of the most intense forms of post-operative pain in all of medicine. This is not said to scare you. It is said so you stop blaming yourself for struggling.
When a surgeon operates on the chest, they have to work through several layers of muscle, spread or sometimes cut through ribs, and reach into the thoracic cavity where your lungs sit. The intercostal nerves, which run along the underside of each rib, are almost always disturbed during this process. These nerves are responsible for a wide band of sensation across your chest wall, which is why pain can feel like it radiates across your whole side rather than being isolated to the incision line.
Pain also comes from the pleural lining, which is the thin membrane that covers your lungs. It is extremely sensitive. Any surgery that touches or opens it causes a significant inflammatory response as it heals.
Here is what most websites completely skip over. When breathing is painful, patients instinctively take smaller, shallower breaths to avoid the discomfort. This feels logical. But it creates a dangerous cycle.
Shallow breathing allows mucus to build up in the lower sections of the lungs. That mucus becomes a breeding ground for bacteria. Within days, this can lead to pneumonia or collapsed lung segments, a condition called atelectasis. Both are serious complications that extend hospital stays and, in vulnerable patients, can be life-threatening.
Painful Truth Suppressing a cough or taking shallow breaths because it hurts is one of the most dangerous things you can do after chest surgery. Controlled, supported breathing and coughing are not just exercises. They are protection against life-threatening complications. |
This is why pain management after thoracic surgery is never just about comfort. It is about giving your lungs the freedom to work properly during healing.
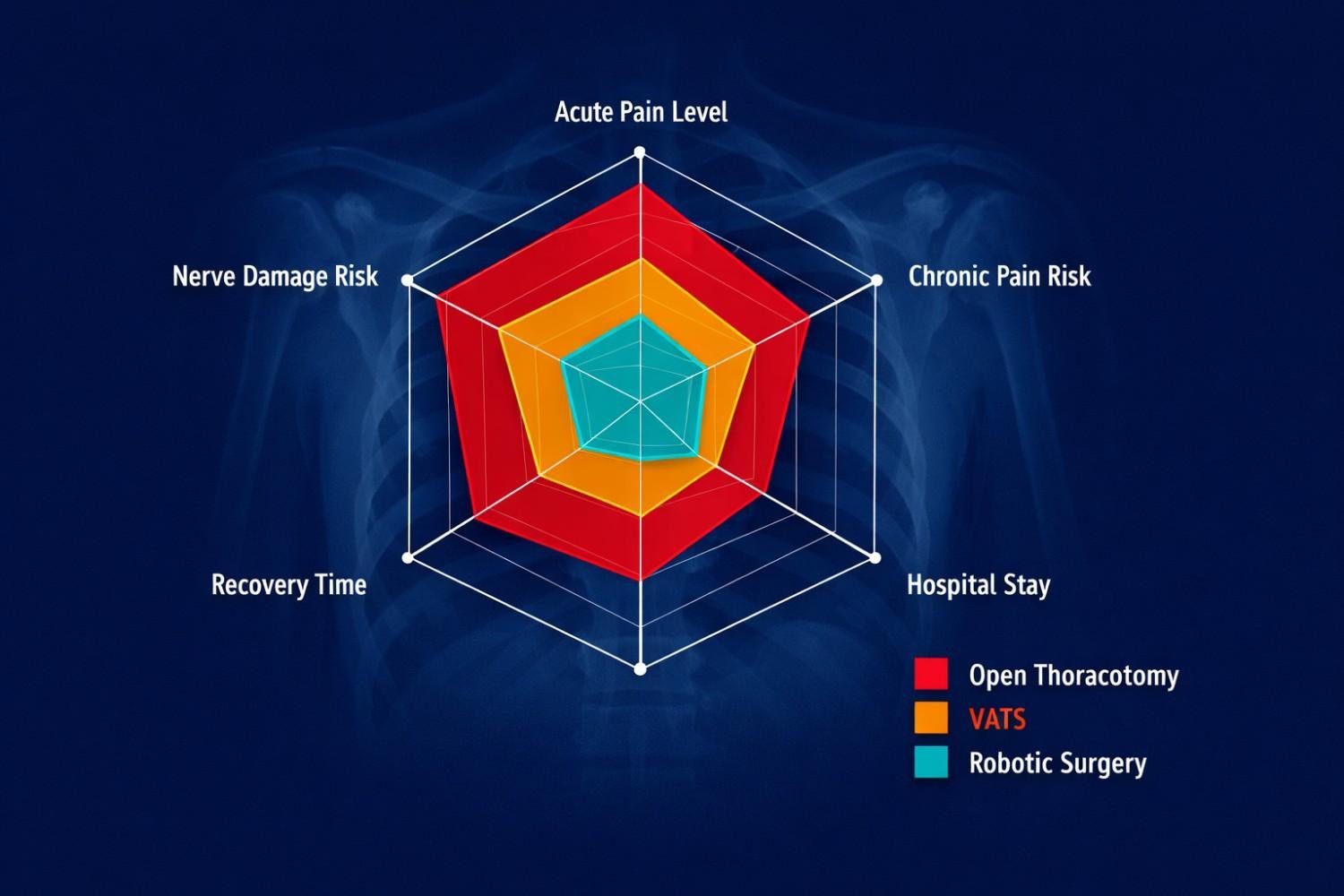
| Factor | Open Thoracotomy | VATS | Robotic Surgery |
| Incision size | Large (10-20 cm) | Small (2-4 cm) | Very small (1-2 cm) |
| Acute post-op pain | High | Moderate | Lowest |
| Chronic pain risk (PTPS) | 38% (higher) | 29% (lower) | Lower still |
| Hospital stay | 5-7 days avg. | 2-4 days avg. | 2-3 days avg. |
| Recovery time | 6-8 weeks | 3-4 weeks | 2-3 weeks |
Source: Journal of Pain and Symptom Management, comparing PTPS incidence by surgical approach (p<0.05)
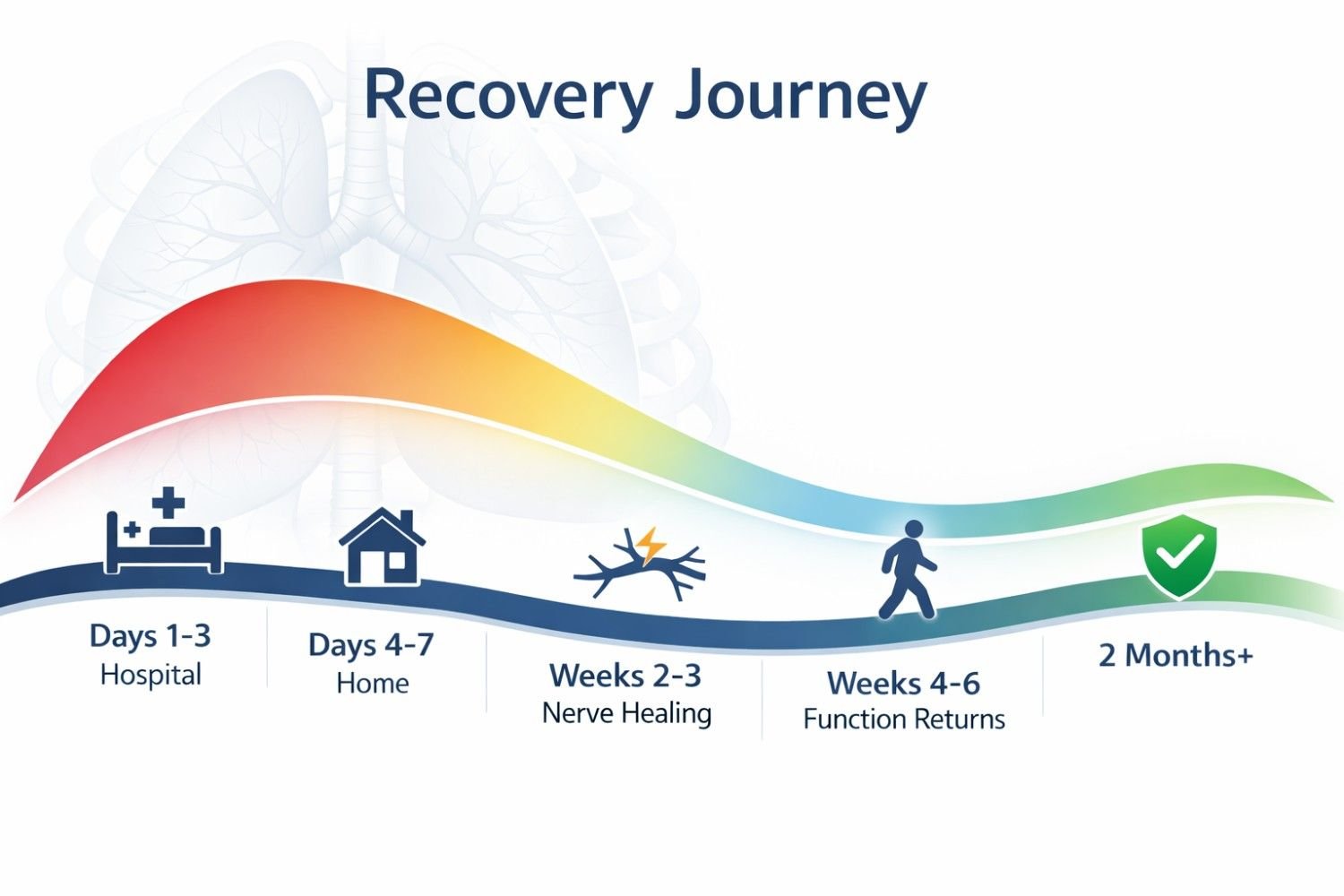
One of the most frustrating things for patients is having no roadmap. You wake up from surgery and you want to know: when will I feel better? Here is an honest, week-by-week picture of what is typical.
Pain is at its peak during these days and will be managed with IV medications or an epidural. You may have a chest tube still in place, which adds significant discomfort. Muscle spasms around the chest are very common. The nursing team will help you use an incentive spirometer (a breathing device) every hour. Accept this help. These early breathing sessions are some of the most important things you can do for your recovery.
You will switch from IV pain control to oral medications. Pain will still be significant but should be slightly more predictable. This is when many patients first notice shoulder pain, which confuses and frightens them. We will address exactly what causes that in the next section. Sleep will be very poor at this stage. Short naps and a semi-reclined sleeping position (elevated 30 to 45 degrees) work better than lying flat.
Most patients experience a shift here. The deep, achy incision pain begins to ease, but a new set of sensations can appear: burning, tingling, electric-zap feelings along the chest wall or around the scar. This is nerve healing, not a sign of new damage. It is the intercostal nerves beginning to regenerate, and it is actually a positive sign, even though it feels strange or alarming.
Most patients are walking regularly, sleeping in more comfortable positions, and stepping down from prescription pain medications toward over-the-counter options. Some numbness or hypersensitivity around the incision site is normal. Physical therapy for shoulder stiffness (very common after chest surgery) should be active at this stage. Patients recovering from chest surgery may also benefit from structured post-surgery physiotherapy in Pune to improve shoulder mobility, reduce stiffness, support breathing exercises, and regain daily movement safely.
Important Milestone If pain at the incision site is still present or returning after 8 weeks, do not assume it is 'just part of recovery.' Pain that persists beyond 2 months after full wound healing may be Post-Thoracotomy Pain Syndrome (PTPS), which is treatable when caught early. |
This is the most under-explained phenomenon in thoracic surgery recovery, and it causes enormous anxiety.
Many patients, just like Sandesh in the story at the start of this article, experience sharp or deep aching pain in the shoulder on the same side as their surgery. It arrives a few days after the operation, often at night. For people who have just had cancer surgery near their heart and lungs, this is terrifying. They assume something has gone very wrong.
In the vast majority of cases, nothing has gone wrong. This is referred pain caused by the phrenic nerve.
The phrenic nerve runs alongside the chest cavity and controls the diaphragm. Surgery in the thoracic region irritates this nerve, and because of how nerve pathways are wired in the human body, the brain interprets that irritation as coming from the shoulder. This is the same mechanism behind the famous left-arm pain of a heart attack. It is a nerve signal detour.
| Likely Referred Nerve Pain (Expected) | Seek Immediate Medical Help |
| Shoulder aches, worse when lying down | Sudden, crushing chest tightness |
| Improves slightly with movement or warmth | Shoulder pain with shortness of breath together |
| Follows pattern of surgical side | Coughing up blood or pink mucus |
| Responds to acetaminophen or NSAIDs | Fainting, sweating, or a feeling of doom |
What most people do not realize is that a significant portion of patients who have open chest surgery go on to develop a condition called Post-Thoracotomy Pain Syndrome (PTPS). This is defined as pain that persists at or near the surgical site for more than 2 months after the operation, once the wound has fully healed.
Studies show that PTPS affects between 33% and 57% of open thoracotomy patients (BJA Education Journal, 2017). About 10% experience pain severe enough to meaningfully limit daily life.
And yet the overwhelming majority of patients who develop this condition do not report it, because they assume chronic pain is just what life looks like after chest surgery. They stay silent. They stop going for walks. They quietly withdraw from activities. They live with something that has real treatment options.
• Intercostal nerve blocks: targeted injections that interrupt the pain signal at its source
• Gabapentin or pregabalin: anticonvulsant medications specifically designed for nerve-based pain
• TENS therapy: small electrical pulses through adhesive pads placed on the chest wall that disrupt pain signaling
• Low-dose antidepressants: certain types (like amitriptyline) are used specifically for chronic neuropathic pain, not for mood
• Spinal cord stimulation: reserved for severe, persistent cases that do not respond to other treatments
Prevention Is Possible Research from the University of Virginia shows that aggressive epidural analgesia immediately after surgery reduces PTPS incidence by up to 50%. Patients who are undergoing thoracic cancer treatment in India should ask their surgeon about regional anaesthesia options before the procedure, not just after. |
Modern pain management after thoracic surgery does not rely on one medication. It layers several approaches together, each targeting a different part of the pain pathway. This reduces the total dose of any single drug and produces better pain control with fewer side effects.
• Acetaminophen (Tylenol/Paracetamol): the backbone of oral pain control; safe to combine with other medications
• NSAIDs like ibuprofen or diclofenac: reduce inflammation directly at the tissue level
• Opioids (tramadol, morphine): used short-term in the immediate post-op period; the goal is to step down from these as fast as safely possible
• Gabapentin or pregabalin: specifically for nerve pain; standard painkillers often fail on this type of pain entirely
• Epidural or nerve block: regional anaesthesia during the hospital phase that directly reduces PTPS risk later
This single technique makes an enormous difference and almost no patient is properly taught it before discharge.
Every time you cough, sneeze, laugh, or get up from a lying position, hold a firm pillow tightly against your chest with both arms. This is called pillow splinting. It reduces the tension across your incision, allows you to cough with enough force to actually clear mucus from your lungs, and dramatically reduces the sharp pain spike that comes with sudden chest movement.
1. Take a slow, deep breath in and hold it for 2 seconds.
2. Press the pillow firmly against your chest.
3. Cough twice in short, controlled bursts.
4. Breathe out slowly.
Do this every hour while awake in your first two weeks at home. It is the single most protective thing you can do against pneumonia after thoracic surgery.
Most patients wait until pain becomes unbearable before taking medication. This is the wrong approach. Pain is much harder to bring back under control once it has peaked.
Keep a simple log, even as a note in your phone, tracking your pain level on a scale of 0 to 10, the time you took medication, and your activity at the time. After a few days, a pattern will emerge. You will see when your pain reliably spikes, and you can take your next dose 30 to 45 minutes before that window. This keeps you consistently comfortable rather than chasing relief.
Bring this log to every follow-up appointment. It gives your doctor specific, actionable information instead of a vague description.
This is an area that the standard medical world almost entirely ignores in recovery guides, particularly for patients pursuing thoracic cancer treatment in Delhi or thoracic cancer treatment in Gurgaon.
The foods you eat in the weeks after surgery have a direct, documented impact on inflammation levels, wound healing speed, and immune function. Here are practical, India-specific recommendations:
• Haldi (Turmeric): curcumin, the active compound in turmeric, is a well-studied anti-inflammatory agent. Add it generously to dal, sabzi, and warm milk with a small amount of black pepper (which increases curcumin absorption by 2,000%).
• Amla (Indian gooseberry): one of the richest natural sources of Vitamin C, which is essential for collagen formation and wound repair
• Adrak (ginger): reduces nausea caused by opioid medications and has its own anti-inflammatory properties
• Protein-rich foods: dal, paneer, eggs, lean chicken, and fish help rebuild muscle and repair tissue; aim for 1.2 to 1.5 grams per kilogram of body weight each day
• Warm water with honey: soothing for the throat and chest, especially in the first two weeks
• Alcohol: interferes directly with pain medications and suppresses immune function
• Highly processed or packaged foods: high sodium content worsens inflammation and fluid retention around healing tissue
• Very cold drinks immediately after surgery: can trigger bronchospasm in sensitive patients
• Excessive raw cruciferous vegetables in week one: cabbage, cauliflower, and broccoli can cause gas and bloating, which increases pressure against a healing chest wall
Here is a scientific fact that surprises most patients: fear and anxiety physically increase the intensity of pain signals in the brain. This is not a metaphor. Brain imaging studies show that a person who is anxious about pain activates a broader set of pain-processing regions than someone who is calm, even when the physical stimulus is identical.
The strongest psychological predictor of chronic pain after surgery is a mental pattern called catastrophizing, which means habitually focusing on worst-case scenarios and feeling helpless about the pain. Research published in the Clinical Journal of Pain found that patients who scored high on catastrophizing before surgery reported significantly more post-operative pain and were more likely to develop PTPS.
This does not mean the pain is 'in your head.' It means that managing your mental state is a legitimate medical tool. Here are practical ways to do it:
• Mindful breathing: the 4-7-8 technique (inhale for 4 counts, hold for 7, exhale for 8) activates the parasympathetic nervous system and reduces perceived pain intensity
• Stay informed: patients who understand what is happening in their body report less fear and less pain; this guide is a step toward that
• Ask your care team about counselling referrals: post-surgical depression is clinically recognised, affects a real proportion of thoracic cancer surgery patients, and responds well to treatment when addressed early
For patients who have undergone surgery for thoracic cancer treatment in India, there is an emotional dimension that clinical guides almost never address. Many patients feel that their body has changed in a fundamental way. Some feel grief over reduced physical capacity, even temporarily. Some fear every twinge is a sign of recurrence.
Family members can help most by listening without minimising. Avoid saying things like 'you should feel grateful the surgery worked.' Instead, let the patient name their experience. Celebrate small milestones together: the first walk to the gate, the first night of decent sleep, the first full meal. Recovery is built one small win at a time.
Most pain after thoracic surgery follows the expected pattern described in this article. But there are specific signals that require immediate action.
Go to Emergency Immediately If You Experience: Sudden severe chest pain combined with shortness of breath | Coughing up blood or bright pink mucus | One leg becoming swollen, red, and painful (possible blood clot) | Lips or fingernails turning blue | Fainting or loss of consciousness | No urine output for 8 or more hours |
Call Your Surgeon's Clinic Same Day If: Pain suddenly increases after steadily improving | Fever rises above 38.5 degrees Celsius | Wound site shows increasing redness, warmth, or discharge | Pain is completely uncontrolled despite all prescribed medications | New tingling or weakness in the legs or torso |
Recovery from thoracic surgery is one of the more challenging journeys a person can face. But it is not a passive process where you simply wait for time to do its work. The patients who recover best are the ones who understand what is happening, use every tool available, and keep communicating openly with their care team.
Here is a quick summary of what this guide covered:
• Pain after thoracic surgery is intense because of nerve and muscle disruption. It is expected, not a sign of failure.
• Shallow breathing and cough suppression are the most dangerous responses to pain. Support your cough with a pillow every time.
• Shoulder pain is usually referred nerve pain, not a cardiac emergency.
• Post-Thoracotomy Pain Syndrome affects up to 50% of open surgery patients and is treatable. Report persistent pain at 8 weeks.
• Pain journaling keeps you ahead of pain waves and makes your follow-up appointments far more productive.
• The foods you eat and the way you manage anxiety are legitimate, scientifically supported tools in recovery.
If you or a family member is navigating recovery after chest surgery, the team led by Dr. Parveen Yadav at Artemis Hospital, Gurgaon, is available for consultations, follow-up appointments, and second opinions. Patients across India and internationally can reach out via call or WhatsApp at +91 9540210956. You do not have to figure this out alone.
Recovery is not a straight line. Some days will be harder than others. But every breath you take fully, every meal that stays down, every step you walk is your body doing the remarkable work of healing. Give it the support it deserves.
What is the one change you can make today, starting with the very next breath you take, to support your recovery?
18+ Yrs Exp | 5,700+ Thoracic & Robotic Cancer Surgeries
Dr. Parveen Yadav is a Director and Senior Consultant in Thoracic and Surgical Oncology, specializing in minimally invasive and robotic lung and esophageal surgeries, with advanced training from AIIMS and Tata Memorial Hospital.
View Full Profile Esophageal Cancer Surgery Recovery Timeline: First Week to 3 Months
Esophageal Cancer Surgery Recovery Timeline: First Week to 3 Months
 Second Opinion for Esophageal Cancer in India: When and Why It Matters
Second Opinion for Esophageal Cancer in India: When and Why It Matters
 Robotic vs Open Esophagectomy: Which Surgery Is Better for Food Pipe Cancer?
Robotic vs Open Esophagectomy: Which Surgery Is Better for Food Pipe Cancer?
Understand the esophageal cancer surgery recovery timeline from the first week to 3 months, including diet, pain, walking, breathing exercises, follow-up, and warning signs.
Learn when to take a second opinion for esophageal cancer in India, what reports to share, and why expert review matters before surgery, chemotherapy, or radiation.
Compare robotic vs open esophagectomy for food pipe cancer. Learn differences in pain, recovery, blood loss, lymph node clearance, hospital stay, cost, and when open surgery may be better.
Copyright 2026 © Dr .Parveen Yadav all rights reserved.
Proudly Scaled by Public Media Solution!