


Ravi was 15 when his mother first noticed it. He had started wearing two t-shirts in May, in the middle of a North Indian summer. He said the layering just felt comfortable. But she had seen the real reason weeks earlier when she walked into his room and saw him standing in front of the mirror, pressing his palm flat against the hollow in the center of his chest. He was not in pain. But he was quietly carrying something heavy.
Their family doctor had told them not to worry. "It is just the way he is built," he said. "He will grow out of it." Three years passed. Ravi did not grow out of it. By 18, he was getting winded walking up two flights of stairs. A specialist finally looked at his chest CT scan and said four words that changed everything: "This needs to be fixed."
Ravi had pectus excavatum, a congenital chest wall deformity where the breastbone grows inward, creating a sunken or caved-in appearance. His sternum had been quietly pressing against his heart for years. And no one had caught it in time.
If this sounds familiar to you or someone you love, you are not alone. And more importantly, there is a solution.

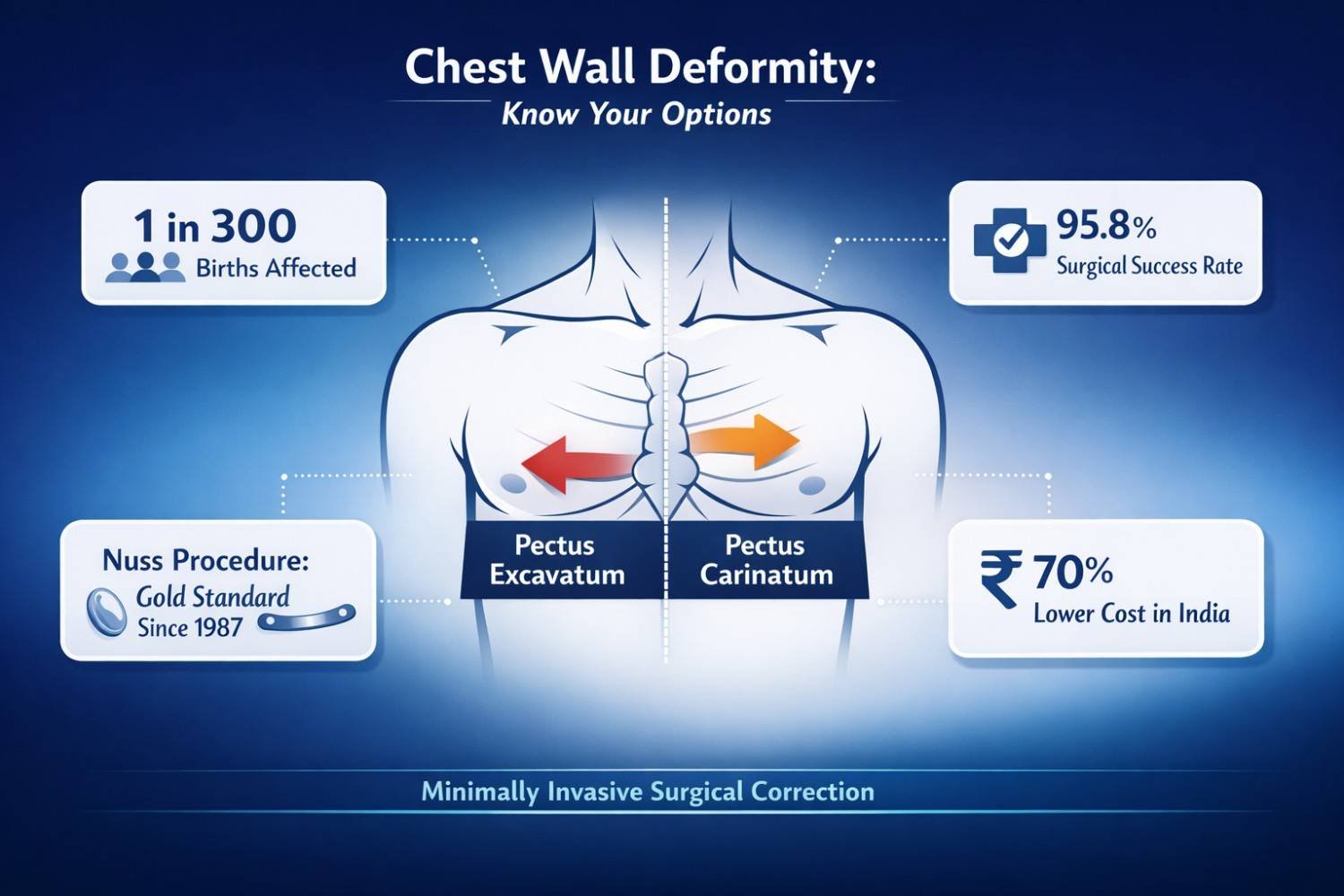
These are the two most common congenital chest wall deformities. Both involve abnormal growth of the rib cartilage and sternum (breastbone), but they move in opposite directions.
Pectus Excavatum (also called sunken chest or funnel chest): The sternum curves inward, creating a hollow in the center of the chest.
Pectus Carinatum (also called pigeon chest or chicken chest): The sternum protrudes outward, creating a noticeable ridge or bump.
Both conditions are present from birth but tend to become more visible and more severe during the teenage growth spurt, which is when most families first seek medical attention.
Pectus excavatum accounts for up to 90% of all chest wall deformities and affects approximately 1 in every 300 to 400 births. Males are affected 3 times more often than females. Source:
Medscape, Pectus Excavatum Overview
Here is the surprising truth that most general physicians miss: pectus excavatum is not just about appearance. When the sternum presses inward far enough, it can directly compress the heart and lungs, affecting how efficiently they function.
• Reduced cardiac output: The heart gets physically pushed to the left or compressed, reducing its ability to pump blood efficiently
• Decreased lung capacity: The lungs cannot expand fully, leading to reduced exercise tolerance
• Frequent respiratory infections: Poor lung expansion creates conditions for recurring infections
• Mitral valve problems: Cardiac anomalies, mainly affecting the mitral and tricuspid valves, have been found in up to one-third of patients referred for pectus repair
• Scoliosis risk: Abnormal chest shape forces the spine to compensate, potentially causing spinal curvature. See: PMC Study on Chest Wall Deformities
Pectus carinatum causes restrictive breathing patterns and postural issues. But what most websites do not mention is that PC patients often experience more severe psychological distress than PE patients. Studies show they report lower satisfaction with their appearance and greater disruption to social and emotional well-being.
A 2026 narrative review published in MDPI confirmed that psychosocial burden, including impaired body image, social anxiety, and low quality of life, is significant in adolescents and young adults with both conditions, often manifesting as social avoidance, concealment behaviors, and emotional distress.
What most people do not realize is that the mental health impact of these conditions is clinically documented and taken seriously by leading surgeons worldwide. It is not drama. It is not teenagers being self-conscious. It is a measurable, real-world health burden.
• Increased social anxiety and avoidance of swimming, sports, locker rooms
• Layering clothes even in warm weather to conceal the chest
• Lower self-esteem and depressive symptoms linked directly to body image distress
• Reduced quality of life even in cases without significant physical symptoms
Research from European Journal of Cardio-Thoracic Surgery found that body image distress was significantly associated with reduced mental quality of life and low self-esteem in both PE and PC patients, with p-values below 0.001. See: Oxford Academic Study
Today, psychological assessment is becoming a standard part of the pre-surgical evaluation at leading thoracic surgery centers. The emotional case for surgery is now treated as equally valid as the physical one.

This is something most competitor websites completely skip over. Knowing how severity is actually measured helps families and patients understand why surgery may or may not be recommended.
The Haller Index is the standard measurement tool for pectus excavatum. It is calculated from a chest CT scan by dividing the internal width of the chest by the shortest distance between the sternum and the spine.
Haller Index Guide:
| Haller Index Score | Severity | Recommendation |
| Below 2.5 | Normal | No treatment needed |
| 2.5 to 3.2 | Mild | Monitor; consider vacuum bell therapy |
| 3.2 to 3.5 | Moderate | Evaluate for surgery |
| Above 3.5 | Severe | Surgery strongly recommended |
| Above 6.0 | Extreme | Urgent surgical consultation |
Source: JTCVS / Aarhus University Study, 2024
Not every case requires surgery. For mild to moderate deformities in growing children, non-surgical approaches can be effective. However, compliance is everything.
• A suction device applied to the chest creates negative pressure, gradually lifting the sternum
• Requires 2+ hours of use daily for 7 to 10 months
• Works best in children under 14 with mild to moderate deformity
• Does not work for asymmetric cases or adults with rigid chest walls
• A custom brace applies external pressure to push the protruding sternum back
• Must be worn 16+ hours daily for best results
• A 2025 retrospective study of 112 patients confirmed significant improvement with good treatment adherence, with deformity height reducing from 1.9 cm to 1.3 cm on average
• Works best in teenagers during active growth phase
When non-surgical options fail, when the deformity is moderate to severe, when cardiac or pulmonary function is affected, or when psychological distress is significant, surgery is the most effective and lasting solution.
Two main surgical procedures are used for chest wall deformity correction in Gurgaon and Delhi. Both are performed by specialized thoracic surgeons with training in minimally invasive techniques.

Developed by Dr. Donald Nuss in 1987, the Nuss procedure, or Minimally Invasive Repair of Pectus Excavatum (MIRPE), has become the globally accepted standard of care. Today, nearly 60% of centers worldwide perform it exclusively. See: PMC / MDPI 2025
Here is how it works, step by step:
• The patient lies on their back under general anesthesia
• Two small incisions are made on each side of the chest wall, a few centimeters long
• A thoracoscopic camera is inserted to guide the surgeon safely around the heart
• A curved metal bar is passed beneath the sternum and flipped to push it outward
• The bar is anchored to the ribs and left in place for 2 to 3 years
• A second short procedure (about 90 minutes) removes the bar once the chest has set in its corrected position
Results: 95.8% of Nuss patients achieved good-to-excellent anatomic outcomes in a review spanning over two decades. Source: ScienceDaily / CHKD Research
The Ravitch procedure is an open surgical technique that involves removing the abnormal rib cartilage and repositioning the sternum. It is chosen when:
• The Nuss procedure is not suitable due to anatomy or prior surgeries
• The deformity is extremely severe (Haller Index above 6.0)
• The patient has had previous chest surgeries that limit bar placement
The Ravitch procedure has a longer recovery but delivers excellent results for the right patients.
Nuss Procedure vs. Ravitch Procedure: A Quick Comparison
| Nuss Procedure (MIRPE) | Ravitch Procedure | |
| Approach | Minimally invasive (keyhole) | Open surgery |
| Incisions | 2 small side incisions | Larger midline incision |
| Cartilage Removal | None | Yes, partial resection |
| Surgery Time | 1 to 3 hours | 2 to 4 hours |
| Hospital Stay | 3 to 5 days | 5 to 7 days |
| Best For | Most PE cases, adolescents & adults | Complex or severe cases, prior surgeries |
| Bar/Implant | Metal bar stays 2 to 3 years | No permanent implant |
| Recovery | Faster, less scarring | Longer, more scarring |
| Success Rate | 95.8% good to excellent outcomes | Excellent for complex cases |
Source: JTCVS, 2024 | PMC Review
For PC, the surgical approach uses the modified Ravitch technique or the Abramson minimally invasive procedure. For complex or mixed PE-PC deformities, a modified sandwich technique uses both internal and external bars to remodel the chest wall in multiple directions. A 2024-2025 retrospective study of 55 patients showed only 5.5% major complication rates and durable correction on long-term follow-up.
• Chest CT scan to calculate the Haller Index
• Pulmonary function tests and echocardiogram (heart ultrasound)
• Psychological screening, increasingly standard at leading centers
• Anesthesia consultation and pre-operative counseling
• Surgery typically takes 1 to 3 hours for the Nuss procedure
• Performed under general anesthesia
• Thoracoscopic camera used throughout to protect the heart
• Blood loss is minimal, typically 10 to 30 mL
• Hospital stay: 3 to 5 days
• Pain management: modern ERAS (Enhanced Recovery After Surgery) protocols introduced in 2024 combine nerve cryoablation and multimodal pain medication, significantly reducing opioid use and hospital stay
• First 6 weeks: no heavy lifting, limited physical activity
• 3 to 6 months: gradual return to sports; aerobic activity is actively encouraged
• 2 to 3 years after: bar removal surgery (about 90 minutes)
• Long-term: normal or near-normal chest contour, improved breathing, better posture, documented improvements in mental health
Source: Enhanced Recovery After Nuss Procedure, Shanghai 2025
India has quietly become a world-class destination for thoracic surgery. The reasons are practical and significant.
• Cost: The Nuss procedure costs $40,000 to $60,000 in the USA. In India, the same procedure is available for $10,000 to $13,500 all-inclusive, a saving of approximately 70%. Source: Medical Tourism Corporation, 2024
• Access to Da Vinci robotic surgery and thoracoscopic techniques at leading hospitals like Artemis Hospital, Gurgaon
• Surgeons trained at institutions like AIIMS New Delhi and Tata Memorial Hospital, Mumbai, with international fellowship credentials
• Full international patient support, from visa assistance to post-operative rehabilitation
• Shorter wait times compared to public health systems in Europe or Canada
If you are looking for the top chest wall tumor surgeon in Gurgaon or a specialist for chest wall deformity correction in Delhi, choosing a center with dedicated thoracic expertise makes all the difference.
• Pectus excavatum and pectus carinatum are not just cosmetic issues. They affect cardiac function, lung capacity, posture, and mental health
• The Haller Index (measured on CT scan) is the standard tool to assess severity and decide on surgical candidacy
• Non-surgical options like vacuum bell therapy and bracing work for mild cases in growing children, but have clear limitations
• The Nuss procedure (MIRPE) is the gold standard for pectus excavatum, with 95.8% good-to-excellent outcomes and a minimally invasive approach
• Psychological improvement post-surgery is clinically documented and sustained long-term
• India offers world-class chest wall deformity correction at 70% lower cost than the USA, with internationally trained surgeons and modern facilities
Dr. Parveen Yadav, Director of Thoracic Surgery and Surgical Oncology at Artemis Hospital, Gurgaon, specializes in minimally invasive and robotic chest wall surgery. As a Da Vinci-certified thoracic surgeon with fellowships from AIIMS New Delhi and Tata Memorial Hospital Mumbai, he has helped hundreds of patients reclaim their confidence and their health.
If you or your child has a chest wall deformity, the most important step is a specialist evaluation. Most families wait years, hoping it resolves on its own. Rarely does it. But when treated correctly, with the right surgeon, at the right time, it resolves completely.
Are you or someone in your family living with an undiagnosed or untreated chest wall deformity? What has been the biggest barrier to getting the right care? We would love to hear from you, and we are here to help.
Book a consultation today or get a free second opinion at chestsurgeryindia.com or call +91 9540210956.
Yes. While adolescence is the optimal window, adults can and do benefit significantly from the Nuss procedure. Research confirms no significant increase in recurrence risk with adult correction. Complications do increase slightly with age and higher Haller Index scores, so earlier evaluation is preferred.
A Haller Index above 3.25 on CT scan, combined with symptoms like shortness of breath, exercise intolerance, chest pain, or documented psychological distress, are the primary criteria. A specialist consultation with a qualified thoracic surgeon is the only way to get a definitive answer.
Pain management has improved dramatically. Modern ERAS protocols with nerve cryoablation and regional blocks have reduced both pain scores and hospital stays. Most patients describe discomfort in the first few days, which is well-managed with medication and improves quickly.
Coverage varies by insurer and policy. When surgery is recommended on clinical grounds (cardiac compression, pulmonary restriction, high Haller Index), it is more likely to be covered. Your surgical team can provide documentation to support an insurance claim.
Pectus excavatum is a sunken chest where the sternum grows inward. Pectus carinatum is a protruding chest where the sternum pushes outward. Both are congenital, both worsen during puberty, and both can be surgically corrected by a qualified thoracic specialist.
1. Medscape: Pectus Excavatum Overview
2. PMC: Epidemiology of Pectus Excavatum and Carinatum (Journal of Thoracic Disease, 2024)
3. PMC: Surgical Treatment of Pectus Excavatum: Pathologic vs Aesthetic (2025)
4. JTCVS: Complication Rates and Haller Index in MIRPE (2024)
5. MDPI: Psychological Impact of Chest Wall Deformities in Adolescents (February 2026)
6. Oxford Academic: Body Image and Quality of Life in PE and PC Patients
7. ScienceDaily / CHKD: Two Decades of Nuss Procedure Outcomes
8. ScienceDirect: Modified Sandwich Technique for Complex Deformities (2024-2025)
9. PubMed: ERAS Protocol for Nuss Procedure, Shanghai (2025)
10. Medical Tourism Corporation: Nuss Procedure Cost in India (2024)
11. CSMEDJ: Non-Surgical Treatment of Pectus Deformities (2025)
18+ Yrs Exp | 5,700+ Thoracic & Robotic Cancer Surgeries
Dr. Parveen Yadav is a Director and Senior Consultant in Thoracic and Surgical Oncology, specializing in minimally invasive and robotic lung and esophageal surgeries, with advanced training from AIIMS and Tata Memorial Hospital.
View Full Profile Esophageal Cancer Surgery Recovery Timeline: First Week to 3 Months
Esophageal Cancer Surgery Recovery Timeline: First Week to 3 Months
 Second Opinion for Esophageal Cancer in India: When and Why It Matters
Second Opinion for Esophageal Cancer in India: When and Why It Matters
 Robotic vs Open Esophagectomy: Which Surgery Is Better for Food Pipe Cancer?
Robotic vs Open Esophagectomy: Which Surgery Is Better for Food Pipe Cancer?
Understand the esophageal cancer surgery recovery timeline from the first week to 3 months, including diet, pain, walking, breathing exercises, follow-up, and warning signs.
Learn when to take a second opinion for esophageal cancer in India, what reports to share, and why expert review matters before surgery, chemotherapy, or radiation.
Compare robotic vs open esophagectomy for food pipe cancer. Learn differences in pain, recovery, blood loss, lymph node clearance, hospital stay, cost, and when open surgery may be better.
Copyright 2026 © Dr .Parveen Yadav all rights reserved.
Proudly Scaled by Public Media Solution!