


Suhas was 54 years old, a non-smoker with clean cholesterol numbers and a cardiologist he trusted. When a dull, nagging ache settled under his left shoulder blade one October morning, he assumed it was the old office chair. He took a painkiller. The ache stayed. Two weeks later, it was still there, not crushing, not dramatic, just there, like a pebble in his shoe that he could not shake out. His cardiologist ran an ECG. Normal. A stress test. Normal. "Your heart is fine," he was told.
Suhas went home relieved. But the pain did not go home with his cardiologist's report. Six weeks later, a CT scan revealed what no heart test had caught: a tumor pressing against the lining of his right lung, on the opposite side from where he thought the pain lived. He had been asking the wrong organ the right question all along.
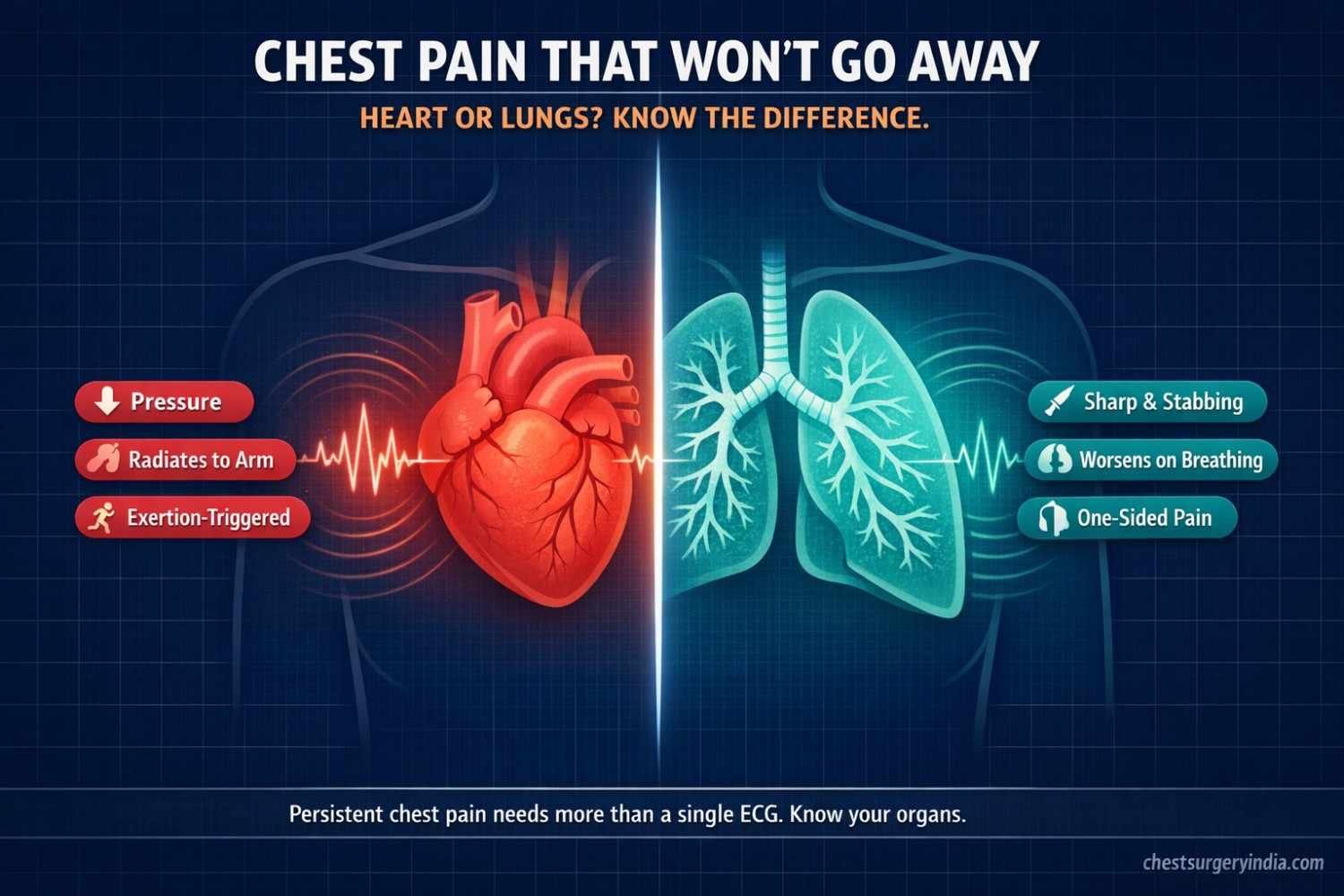
This story is more common than most people realize. Chest pain that won't go away is one of the most searched health concerns online, and one of the most misunderstood. Most people immediately think heart attack. But the chest is a crowded neighborhood. The heart and lungs share the same address and, crucially, the same nervous system pathways, which means pain coming from one can feel like it is coming from the other.
Persistent chest pain is any chest discomfort that lasts beyond a few days without a clear diagnosis. It can come from the heart, lungs, pleura, esophagus, or even a growing tumor, and it deserves more than a single ECG.
Here is the surprising truth about chest pain: the heart, lungs, esophagus, and major blood vessels all share the same thoracic autonomic nerve pathways. According to the Merck Manual, because nerve fibers overlap in the dorsal ganglia, a painful signal from any of these organs can be felt anywhere between the ear and the belly button, including the arms. This is called referred pain, and it is the reason a lung tumor pressing on a nerve can feel exactly like angina.
The numbers are eye-opening. Chest pain is the second most common reason for emergency department visits in the US, accounting for nearly 11 million encounters every year. Yet fewer than 10% of those patients are ultimately diagnosed with acute coronary syndrome (ACS), meaning a heart-related cause. The rest have lung problems, digestive issues, musculoskeletal pain, or conditions that require a very different type of specialist.
The cost of this diagnostic confusion is staggering: diagnostic testing for chest pain in the US alone costs an estimated $10 to $13 billion annually. But the real cost is time, specifically the weeks or months patients spend in the wrong diagnostic lane while the real cause quietly progresses.
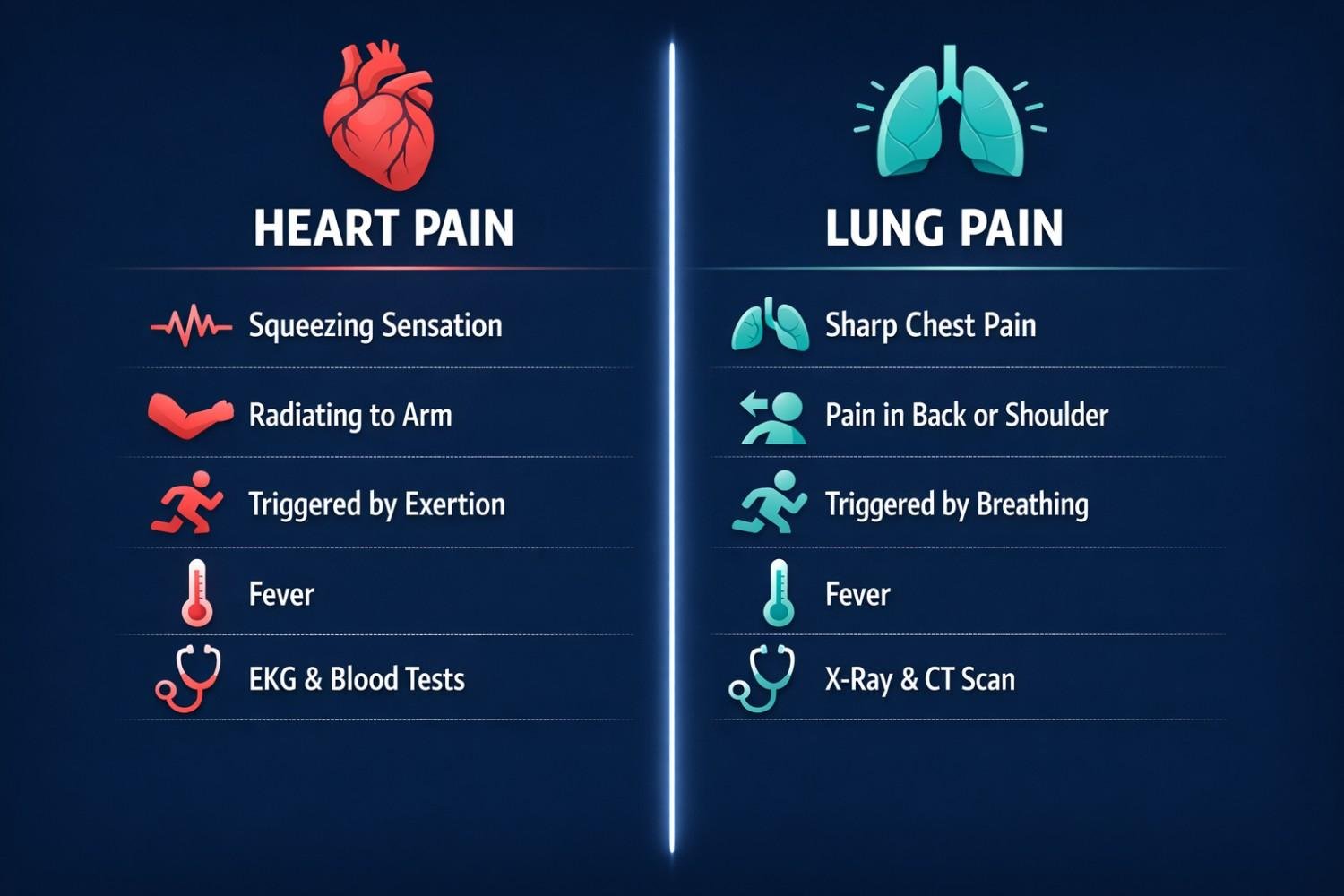
Heart-related chest pain typically feels like pressure, squeezing, tightness, or heaviness in the center of the chest. Many patients describe it as an elephant sitting on their chest. It is usually triggered by physical exertion or emotional stress and goes away with rest. It can radiate to the left arm, jaw, neck, or upper back.
According to Harvard Health Publishing, only about 20% of patients who visit hospital emergency departments for chest pain are diagnosed with a heart attack or unstable angina. This means the vast majority of people walking in with chest pain are experiencing something else entirely.
Common cardiac causes include:
• Heart attack (acute myocardial infarction)
• Angina, where plaque buildup narrows the coronary arteries and reduces blood flow
• Pericarditis, an inflammation of the sac surrounding the heart
• Aortic dissection, a tear in the inner wall of the aorta that causes a tearing pain radiating to the back
What most people do not realize is that women often experience cardiac chest pain very differently. Men tend to get the classic "elephant on the chest" presentation. Women are more likely to have fatigue, nausea, shortness of breath, and chest discomfort that does not follow the standard exertion-rest pattern. This condition, called microvascular angina, affects the small blood vessels of the heart and can be missed entirely on standard stress tests.
Lung-related chest pain has a distinct fingerprint. It is usually sharp and stabbing, and it gets worse when you breathe in, cough, or laugh. This is called pleuritic chest pain, and it comes from inflammation of the pleura, the two-layer membrane that wraps around the lungs and lines the inside of the chest wall. When those two layers get irritated and rub against each other, the result is a friction-rub pain that is almost impossible to confuse with a heart attack once you know what to look for.
According to the American Academy of Family Physicians, pulmonary embolism (PE), a blood clot in the lungs, is the most common serious cause of pleuritic chest pain, found in 5% to 21% of patients who arrive at the emergency department with this type of pain. PE requires immediate treatment, so this is not a symptom to brush off.
Other lung conditions that cause persistent chest pain include:
• Pleurisy: inflammation of the pleural lining from infection, autoimmune disease, or viral illness
• Pneumonia: chest pain with fever, productive cough, and sometimes consolidation in the lung
• Pneumothorax: a collapsed lung, which causes sudden, sharp one-sided pain with breathlessness
• Empyema: a pocket of infected fluid in the pleural space that causes severe chest pain with high fever and requires surgical drainage
• Lung cancer: as tumors grow and press on surrounding structures, they cause persistent, worsening chest discomfort
Here is what the standard "heart vs. lungs" articles consistently leave out: lung cancer can cause two very specific pain patterns that are frequently misdiagnosed for months.
Pancoast tumor pain: A tumor at the very top (apex) of the lung can grow silently without causing a cough or breathing problems. Instead, it presses on nearby nerves and causes severe shoulder pain, arm pain, and even weakness or numbness in the hand. This is so commonly mistaken for a cervical spine problem or frozen shoulder that some patients go through months of physiotherapy before a chest CT scan reveals the real cause. According to the American Cancer Society, Pancoast tumors can also sometimes cause severe shoulder pain by pressing on the brachial plexus nerve bundle.
Superior Vena Cava (SVC) syndrome: When a lung tumor presses on the superior vena cava, the large vein carrying blood from the head and arms to the heart, it causes swelling in the face, neck, and arms, sometimes with a bluish-red skin color. This is accompanied by chest pain, headaches, and dizziness. It can develop gradually, but in some cases it becomes life-threatening. If you see someone with facial swelling plus chest pain, this needs emergency evaluation, not a wait-and-see approach.
Use this quick-reference table to understand the key differences at a glance.
| Feature | Cardiac (Heart) | Pulmonary (Lungs) |
| Pain quality | Pressure, squeezing, heaviness | Sharp, stabbing, burning |
| Worsens with breathing? | No | Yes - key differentiator |
| Radiates to arm/jaw? | Yes - left arm, jaw, neck | Usually no |
| Triggered by exertion? | Yes - classic angina pattern | Sometimes - PE or empyema |
| Accompanied by cough? | Rarely | Very common |
| Fever present? | Unlikely | Yes - pneumonia, empyema |
| Improves leaning forward? | No | Yes - pericarditis overlap |
| One-sided localization? | Central or left-sided | Can be one-sided |
| Key emergency test | ECG + Troponin | CT Pulmonary Angiography (CTPA) |
Important note: These are general patterns, not a diagnostic tool. A normal ECG does not rule out a lung cause. Always seek professional evaluation.
Chest pain that keeps returning after cardiac tests come back normal? It could be a lung or pleural condition. Book a consultation with Dr. Parveen Yadav -- Thoracic Surgeon at Artemis Hospital, Gurgaon -- for a specialist evaluation. |
Some conditions blur the line between cardiac and pulmonary pain so thoroughly that even experienced emergency physicians find them challenging. Here is what makes the middle ground so dangerous.
Pulmonary embolism is a lung problem that acts like a heart problem. When a blood clot travels to the lungs and blocks blood flow, it causes pleuritic chest pain from the lung side and puts severe strain on the right side of the heart simultaneously. Patients often present with sudden breathlessness, one-sided chest pain, a racing heartbeat, and sometimes a feeling of impending doom. This is a medical emergency with a time-sensitive window for treatment with blood thinners or, in severe cases, clot-removal surgery.
Pericarditis (inflammation of the sac around the heart) is often confused with pleurisy. Both cause sharp chest pain. The key differentiator is body position:
• Pericarditis pain improves when the patient sits up and leans forward, and it worsens when lying flat
• Pleuritic pain worsens specifically during inhalation, not based on body position
Missing this difference means treating the wrong organ. Getting it right changes the entire treatment approach.
In advanced lung cancer, a tumor near the heart can press on or invade the pericardium, causing pain that mimics cardiac angina. This is one reason why patients with known heart disease should still have a thoracic evaluation if their chest pain pattern changes or stops responding to cardiac medication. A change in pain character is always a red flag worth investigating.
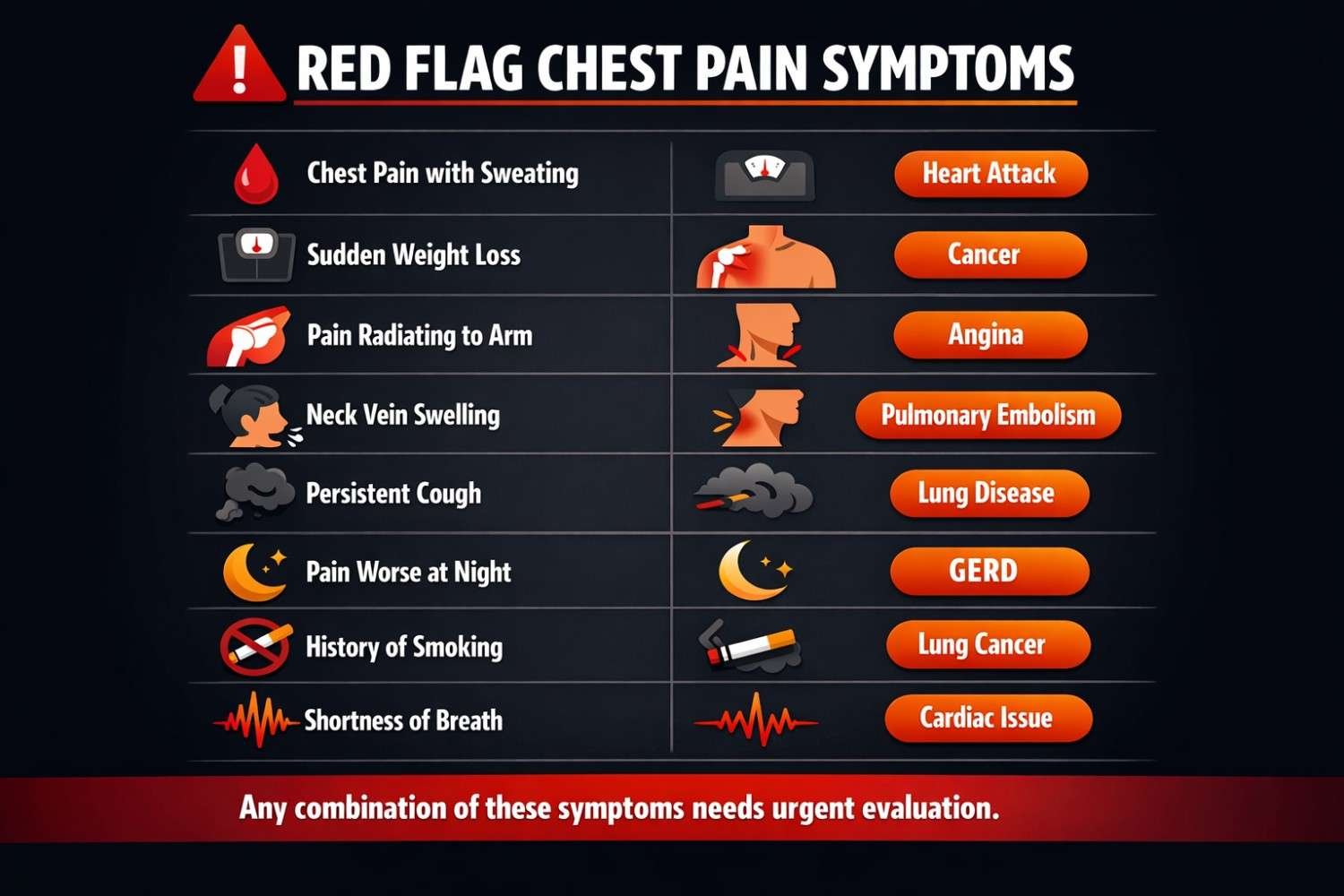
The following symptom combinations should be treated as urgent, not as something to monitor at home.
| Red Flag Symptom | Possible Condition |
| Chest pain + blood in sputum | Lung cancer, pulmonary embolism |
| Chest pain + unexplained weight loss | Lung cancer, mesothelioma |
| Shoulder/arm pain with no injury history | Pancoast tumor (lung apex cancer) |
| Face, neck, or arm swelling + chest pain | Superior Vena Cava (SVC) syndrome - lung tumor |
| Persistent cough 3+ weeks + chest ache | Lung cancer, chronic infection |
| Chest pain worsening at night or lying flat | Pericarditis, pleural effusion, mediastinal mass |
| Smoker 50+ years with new chest pain | Lung cancer screening needed urgently |
| Chest pain + hoarse voice | Lung tumor pressing on recurrent laryngeal nerve |
The American Thoracic Society specifically recommends seeking evaluation if you develop new shortness of breath, chest pain, fever, chills, or unexplained weight loss of 10 pounds or more, especially if you are a smoker or have had a prior lung scan showing a nodule.
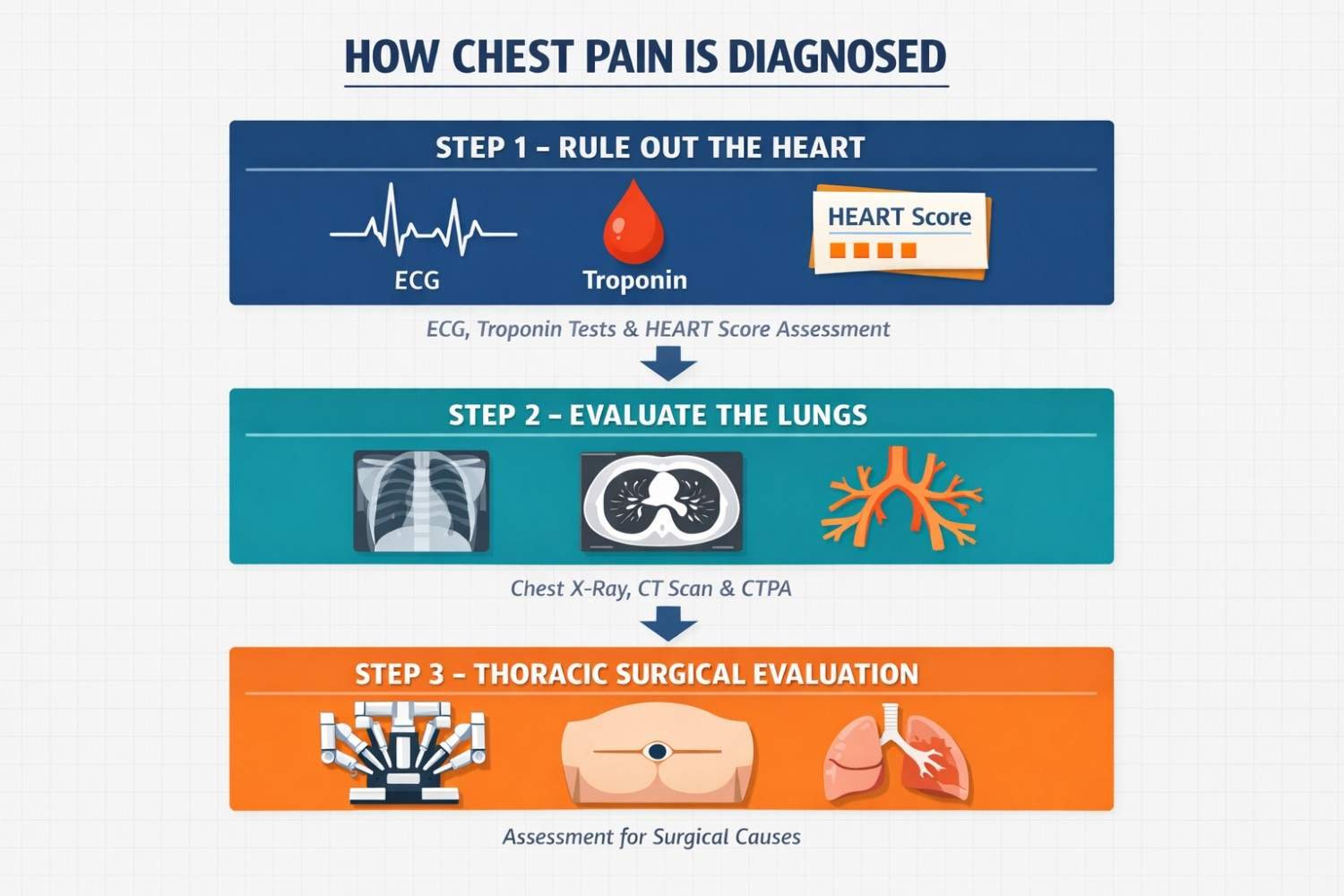
The first priority in any emergency chest pain evaluation is to rule out a heart attack. Doctors use an ECG (electrocardiogram) to check for electrical changes in the heart, and a high-sensitivity cardiac troponin blood test to detect any damage to heart muscle. The HEART Score, developed in 2008, is a clinical risk tool that ER doctors use to classify patients as low, moderate, or high cardiac risk based on five factors: History of the pain, ECG findings, Age, Risk factors (smoking, diabetes, hypertension), and Troponin levels. Low-risk patients can often be safely discharged; high-risk patients need urgent treatment.
What most people do not realize is this: a normal ECG and a normal troponin level do not mean the lungs are clear. These tests only evaluate the heart. If cardiac causes are ruled out, a separate lung-focused workup is always needed.
The main diagnostic tools for lung-origin chest pain include:
• Chest X-ray: First-line imaging for pneumonia, collapsed lung, pleural effusion, and obvious masses
• CT Pulmonary Angiography (CTPA): The gold standard test for pulmonary embolism, per StatPearls / NCBI
• High-Resolution CT (HRCT): Detects lung nodules, tumors, interstitial lung disease, and mediastinal masses with much greater precision than an X-ray
• PET-CT scan: Identifies metabolically active tumors and checks if cancer has spread to lymph nodes or other structures
• D-dimer blood test: A screening tool for pulmonary embolism; elevated levels prompt further imaging
Many patients with persistent, unexplained chest pain are sent home after a normal ECG and X-ray with no further investigation. If the pain continues beyond two to three weeks with no diagnosis, a CT scan of the chest is the next logical step.
This is the section that almost no online chest pain article ever includes, yet it is the most important step for a significant group of patients.
Most people with persistent chest pain follow a path from cardiologist to gastroenterologist to pulmonologist. The thoracic surgeon is rarely on the list. But there are specific scenarios where a thoracic surgical evaluation is not optional, it is essential.
• A CT scan reveals a lung nodule, mass, or suspicious shadow that needs biopsy or removal
• You have a pleural effusion (fluid around the lungs) requiring drainage or tissue sampling
• You have been diagnosed with empyema (infected fluid in the pleural space) that is not responding to antibiotics
• A mediastinal mass or enlarged lymph nodes are causing pressure symptoms in the chest
• Lung cancer has been confirmed and surgical resection is being considered
• You have chest wall tumor, esophageal cancer, or tracheal disease that needs specialist surgical management
• Bronchopleural fistula, a connection between the airway and pleural space, is causing persistent symptoms
One of the biggest advances in thoracic medicine over the last decade is the widespread availability of minimally invasive thoracic surgery. Video-Assisted Thoracoscopic Surgery (VATS) and robotic-assisted surgery allow surgeons to operate through small keyhole incisions rather than opening the entire chest wall. This means shorter hospital stays, significantly less post-operative pain, faster recovery, and better quality of life after surgery compared to traditional open thoracotomy. If a lung cause is confirmed for your persistent chest pain, the surgical options today are far less daunting than they were even 10 years ago.
Diagnosed with a lung nodule, pleural effusion, or mediastinal mass? Do not delay a specialist opinion. Explore your surgical options with a specialist in minimally invasive thoracic surgery. Book a second opinion today. |
Your history and habits significantly affect what type of chest pain you are most likely to have.
• Smoking history: The most important risk factor for lung-origin chest pain. Lung cancer is responsible for approximately 90% of smoking-related cancer deaths, per the CDC. Any smoker over 50 with new or worsening chest pain needs an urgent chest CT, not just reassurance.
• Long-haul travel or prolonged immobility: Major risk factors for deep vein thrombosis (DVT) and pulmonary embolism. If you have chest pain within 2 to 3 weeks of a long flight or hospital admission, PE must be ruled out promptly.
• Recent respiratory infection: Post-viral pleurisy or pericarditis can develop after COVID-19, influenza, or other chest infections, causing lingering chest pain for weeks after the acute illness resolves.
• Autoimmune conditions: Conditions like lupus, rheumatoid arthritis, and sarcoidosis can cause pleuritis (pleural inflammation) or pericarditis, resulting in ongoing chest pain that does not fit a standard cardiac or pulmonary mold.
• Anxiety and panic disorder: Panic attacks genuinely cause chest pain, rapid heartbeat, and shortness of breath. This is a real physical response, not imaginary. However, anxiety should only be diagnosed after cardiac and pulmonary causes have been fully excluded, not as a default explanation.
Follow this step-by-step approach:
1. If the pain is severe, sudden, or crushing: Call emergency services immediately. Do not drive yourself.
2. If the pain is persistent but not acute: Do not wait months hoping it will resolve. See a doctor within days.
3. Get an ECG and high-sensitivity troponin test to rule out cardiac causes first.
4. If cardiac tests are normal but pain continues: Request a chest CT scan, not just an X-ray.
5. Ask your doctor directly: 'Has a lung cause been fully evaluated?'
6. If a nodule, mass, or pleural abnormality is found on imaging: Seek a thoracic surgical consultation. Early intervention in lung cancer dramatically improves outcomes.
• Chest pain that does not go away deserves a thorough evaluation, not just a single ECG
• Heart-related pain typically feels like pressure or squeezing and is triggered by exertion; lung-related pain is usually sharp and worsens with breathing
• A normal cardiac test does not mean the lungs are clear, they need their own workup
• Pancoast tumors and SVC syndrome are lung cancer presentations that masquerade as shoulder or vascular problems for months
• Pulmonary embolism is the most serious common cause of pleuritic chest pain and a medical emergency
• If a lung or chest cause is confirmed, minimally invasive thoracic surgery offers effective, modern treatment with faster recovery
Persistent chest pain is your body asking a question. The only wrong answer is to ignore it.
If your cardiac tests have come back normal but the pain keeps returning, it may be time to ask whether your lungs have been fully evaluated. Have you had a chest CT scan yet, and if not, what is stopping you?
Dr. Parveen Yadav is a Da Vinci-certified robotic thoracic surgeon and Director of Thoracic Surgery & Surgical Oncology at Artemis Hospital, Gurgaon. If your chest pain has no cardiac explanation, do not wait. Request a consultation for lung cancer treatment in Gurgaon and get the specialist evaluation your symptoms deserve. |
Yes. A lung tumor pressing on the pericardium (the sac around the heart) or on the intercostal nerves can create pain that mimics cardiac angina. The absence of typical cardiac risk factors and a normal ECG should prompt lung imaging in these cases.
Pleuritic pain is sharp and stabbing and gets noticeably worse with every breath. Cardiac pain is more of a pressure, squeezing, or heaviness, often triggered by exertion. The breathing-related worsening is the single most useful differentiator.
Yes. Any chest pain lasting more than a few days without a clear diagnosis should be evaluated by a doctor. Two weeks of persistent pain without a diagnosis is always worth an urgent review, especially if it is accompanied by any of the red flags listed in this article.
A Pancoast tumor is a type of lung cancer that develops at the very top (apex) of the lung. Because of its location, it grows near the nerves that supply the shoulder, arm, and hand. This causes shoulder pain, arm pain, and sometimes hand weakness or numbness, which is why it is so often misdiagnosed as a musculoskeletal problem. A chest CT scan is the only reliable way to identify it.
Surgery becomes necessary when the cause of chest pain is a lung tumor, a pleural mass, empyema (infected pleural fluid) not responding to antibiotics, mediastinal masses, or a bronchopleural fistula. The good news is that many of these conditions can now be treated using minimally invasive VATS or robotic thoracic surgery, which significantly reduces recovery time and post-operative discomfort.
18+ Yrs Exp | 5,700+ Thoracic & Robotic Cancer Surgeries
Dr. Parveen Yadav is a Director and Senior Consultant in Thoracic and Surgical Oncology, specializing in minimally invasive and robotic lung and esophageal surgeries, with advanced training from AIIMS and Tata Memorial Hospital.
View Full Profile Esophageal Cancer Surgery Recovery Timeline: First Week to 3 Months
Esophageal Cancer Surgery Recovery Timeline: First Week to 3 Months
 Second Opinion for Esophageal Cancer in India: When and Why It Matters
Second Opinion for Esophageal Cancer in India: When and Why It Matters
 Robotic vs Open Esophagectomy: Which Surgery Is Better for Food Pipe Cancer?
Robotic vs Open Esophagectomy: Which Surgery Is Better for Food Pipe Cancer?
Understand the esophageal cancer surgery recovery timeline from the first week to 3 months, including diet, pain, walking, breathing exercises, follow-up, and warning signs.
Learn when to take a second opinion for esophageal cancer in India, what reports to share, and why expert review matters before surgery, chemotherapy, or radiation.
Compare robotic vs open esophagectomy for food pipe cancer. Learn differences in pain, recovery, blood loss, lymph node clearance, hospital stay, cost, and when open surgery may be better.
Copyright 2026 © Dr .Parveen Yadav all rights reserved.
Proudly Scaled by Public Media Solution!