


Rajan was 52 years old when he first noticed the cough. It had been there for almost three months, quiet but persistent, like a guest who wouldn't leave. His local doctor looked at his chest X-ray, pointed to a white shadow in the upper right lobe, and told him with confident simplicity: "Looks like TB. Let's start treatment."
Rajan completed six full months of anti-tuberculosis drugs. He endured the nausea, the fatigue, the follow-up appointments. And when the course ended, the cough remained. So did the shadow.
By the time Rajan reached a chest specialist in Gurgaon, the shadow had a name. It was Stage III lung cancer. Not tuberculosis. The six months of TB treatment had done nothing except allow the tumor to grow while the clock ran out.
Rajan's story is not rare. In India, where tuberculosis and lung cancer share strikingly similar symptoms and nearly identical X-ray patterns, this kind of diagnostic confusion happens far more often than most people realize.
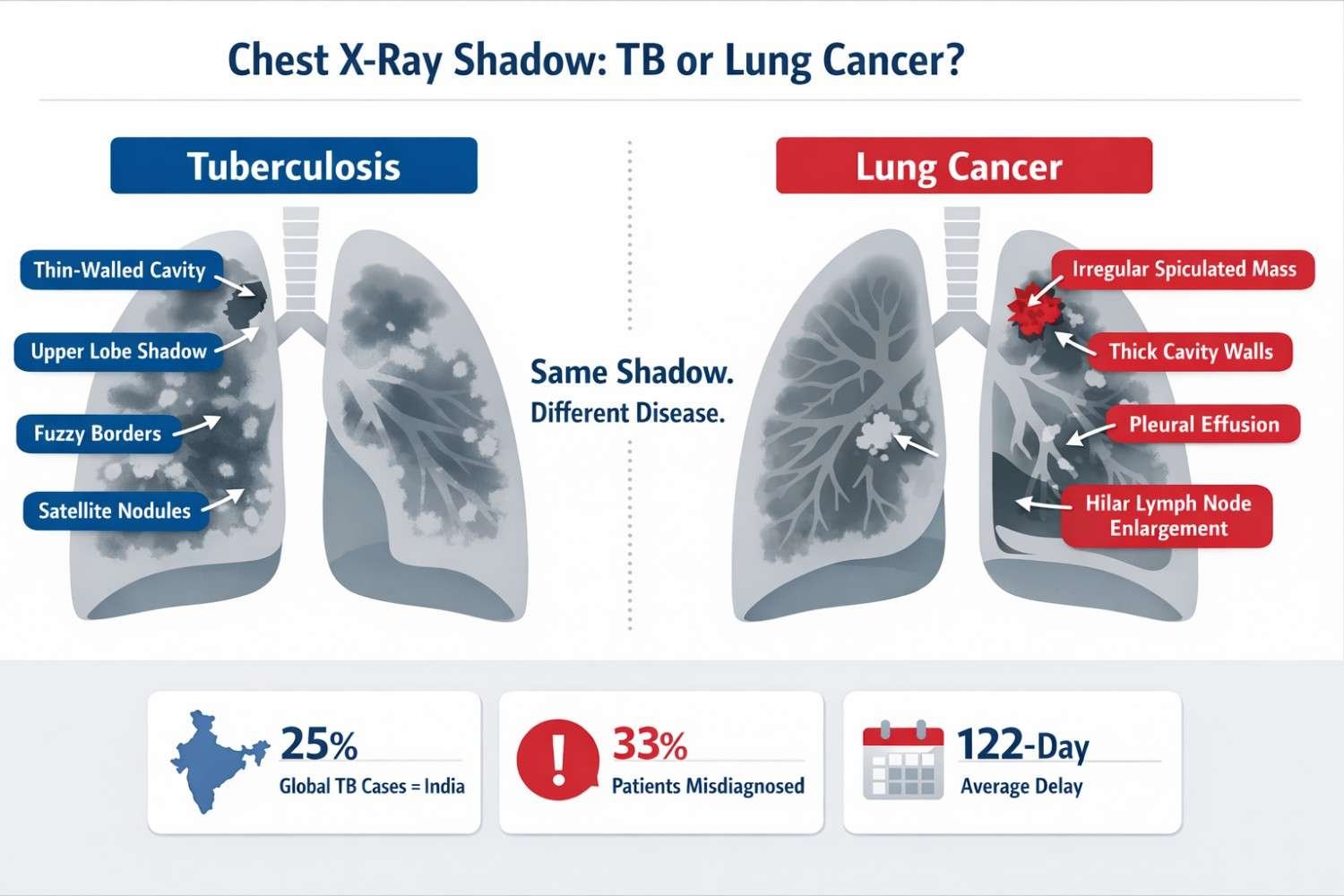
A chest X-ray shadow is any area on the scan that appears whiter or grayer than normal lung tissue (which should look dark). It can represent infection, inflammation, fluid, scar tissue, or a tumor. That single description covers both tuberculosis and lung cancer, which is exactly why it creates so much confusion.
India carries a uniquely high burden of both diseases simultaneously. That double burden is what makes getting the diagnosis right so critical.
According to the WHO Global Tuberculosis Report 2025, India accounts for 25% of all tuberculosis cases globally in 2024. TB returned as the world's leading infectious disease killer in 2023, surpassing COVID-19.
At the same time, lung cancer cases in India are projected to reach over 111,000 by 2025 according to the National Cancer Registry Programme (ICMR). Lung cancer in India also tends to appear almost a decade earlier than it does in Western countries, with patients presenting between ages 54 and 70.
Here is the number that shocks most people: Studies published in Lung India and JCO Global Oncology report that between 18% and 33.6% of lung cancer patients in India received anti-tuberculosis treatment (ATT) before their cancer was correctly diagnosed. That is not a rare exception. That is a documented, repeated pattern.
STAT THAT MATTERS In one North India study, the average delay between a patient's first symptoms and their definitive lung cancer diagnosis was 91 days. In cases involving wrongful ATT, that delay extended even further, reaching 122 days from primary doctor referral to specialist care. (Source: Lung India, PMC 2022) |
That kind of delay is not just a number. In lung cancer, stages matter enormously. A Stage I cancer has a very different treatment outcome than Stage III or IV. Every month of missed diagnosis changes survival odds.
Not sure if your chest shadow is TB or something more serious? Get a specialist review before starting any treatment. Book a Free Second Opinion with Dr. Parveen Yadav →
Before understanding how doctors tell the two conditions apart, it helps to understand what a shadow actually represents on an X-ray.
In a healthy chest X-ray, the lungs appear mostly dark because they are filled with air, which lets X-rays pass through easily. When something denser fills part of the lung, whether fluid, pus, scar tissue, or a tumor, that area absorbs more radiation and shows up lighter. That lighter area is the shadow.
Here is the reassuring part: the vast majority of shadows are not cancer. According to data from the American Thoracic Society, fewer than 5% of detected pulmonary nodules turn out to be malignant. Shadows can appear from healed infections, old TB scars, fluid buildup, benign growths, or inflammation.
But that also means you cannot look at a shadow and make a safe assumption either way. The concern lies in getting the diagnosis right, not in panicking prematurely.
Types of Shadows That Appear on a Chest X-Ray
| Shadow Type | What It Looks Like | Common Causes |
| Consolidation | Dense white area replacing dark lung | TB, pneumonia, lung cancer, atelectasis |
| Nodule (under 30mm) | Small round white spot | Healed infection, TB granuloma, early cancer |
| Mass (over 30mm) | Large, often irregular white opacity | Lung cancer until proven otherwise |
| Cavitation | White ring with dark hollow center | TB abscess, cavitating lung cancer |
| Miliary Pattern | Tiny scattered nodules in both lungs | Miliary TB, blood-borne cancer spread |
| Ground-Glass Opacity | Hazy cloud-like area, vessels still visible | Adenocarcinoma, COVID-19, early TB |
| Pleural Effusion | White opacity at lung base (fluid) | TB, lung cancer, heart failure |
Source: Radiology Assistant | Indographics 2024
Tuberculosis is notoriously unpredictable on imaging. I often tell patients and referring physicians the same thing: TB can wear almost any costume on a chest X-ray. It can look like a nodule, a mass, a cavity, or even a diffuse infection. This radiological chameleon quality is precisely what makes it so dangerous to assume.
According to a 2024 review published in Indographics, TB lesions on imaging fall into five main categories:
• Parenchymal disease: Dense patches of consolidation, classically in the upper lobes. They can appear cloud-like when active or nodular when chronic.
• Cavitation: A hollow area surrounded by a white ring. The walls in TB cavities tend to be thinner and smoother than cancer cavities.
• Lymph node enlargement: Visible as hilar (lung root) swelling, especially common in younger patients with primary TB.
• Miliary pattern: Tiny 1-2mm nodules scattered uniformly through both lungs, like millet seeds, from blood-borne TB spread.
• Pleural effusion: Fluid accumulation, often on the left side, causing a white base on the X-ray.
The Hidden TB Clue That Most Blogs Miss: The Tree-in-Bud Pattern
On CT scan (not plain X-ray), active TB produces a very distinctive appearance called the tree-in-bud pattern. This refers to centrilobular nodules that branch out like small budding trees. When a radiologist spots this pattern, it is a strong signal of active endobronchial TB spread.
There is also the Ghon Focus, a calcified, dense, bone-white nodule that marks a healed old TB infection. It sits quietly in the lung periphery for decades and does not indicate active disease. But here is what most people never get told: an old TB scar like this can become the birthplace of lung cancer later in life. More on that shortly.
Here is the surprising truth about lung cancer on X-ray: a plain chest X-ray misses up to 25% of lung cancers, especially when tumors are small, positioned behind ribs, or located near the heart. That is a significant limitation that patients and families rarely hear about. A clear X-ray does not guarantee a healthy lung.
Tumors smaller than 5-6mm in diameter are often invisible on a plain X-ray. On modern CT scans, however, lesions as small as 1-2mm can be detected. This is one of the most important reasons why a suspicious X-ray shadow must always be followed up with a CT scan and specialist evaluation. Source: PMC / Pulmonary TB as Differential Diagnosis of Lung Cancer.
When lung cancer does show on a chest X-ray, the mass tends to have these distinguishing features:
• Irregular, spiky (spiculated) borders with radiating strands, like a star shape at the edges of the white area
• Thicker cavity walls if cavitation is present, with irregular inner surfaces
• A single dominant mass rather than scattered nodules
• Possible collapse of nearby lung tissue if the tumor is blocking an airway
• Enlarged lymph nodes at the lung root (hilar) or in the chest (mediastinal), seen as widening
• Pleural effusion (fluid around the lung), often large and on the right side
Experienced thoracic surgeons and oncologists do not rely on the X-ray alone. Diagnosis of any chest shadow is a layered process that combines patient history, symptoms, imaging, blood tests, and ultimately tissue analysis. Here is how that works in practice.
Step 1: Patient History Tells Half the Story
Before I even look at the scan, the patient's history gives me critical clues. Risk factors for TB and lung cancer are different enough that they can point the diagnosis in a clear direction early on.
| Suggests Tuberculosis | Suggests Lung Cancer |
| Known contact with TB patient | Age above 50 with heavy smoking history |
| Gradual weight loss over months | Sudden, significant unexplained weight loss |
| Low-grade evening fever pattern | Non-specific fever with no clear pattern |
| Positive IGRA or tuberculin skin test | Cough that changed character or worsened |
| Low income, overcrowded living conditions | Exposure to asbestos, radon, or industrial fumes |
| Young patient (under 40) | Family history of lung cancer |
| Responds partially to antibiotics | No improvement on antibiotics or ATT course |
| HIV positive or immunocompromised | Swelling in face, arms, or distended neck veins |
Step 2: Symptom Patterns That Are Easy to Confuse
Both diseases cause cough, weight loss, fatigue, and hemoptysis (coughing blood). But the quality and timeline of those symptoms often differ in ways that guide diagnosis:
Fever pattern: TB causes low-grade evening-rise fever. Lung cancer fever has no predictable pattern.
Weight loss: TB causes gradual loss. Lung cancer causes sudden, pronounced loss.
Cough: Any new cough persisting beyond 2 weeks in a smoker over 40 should raise immediate suspicion for lung cancer, not just TB.
Hoarseness: Commonly seen in lung cancer when the tumor involves the nerve near the voice box. Rare in TB.
Bone pain or neurological symptoms: These suggest cancer that has spread to bones or the brain. TB does not typically cause these.
Step 3: Reading the X-Ray and CT Scan Carefully
The imaging features that distinguish TB from lung cancer are subtle but learnable. A plain chest X-ray is the starting point. A CT scan is always the essential next step for any shadow that does not have an obvious, confirmed cause.
| Imaging Feature | Tuberculosis | Lung Cancer |
| Lesion location | Upper lobes (classic); can appear anywhere | Any lobe; peripheral or central |
| Border appearance | Fuzzy, ill-defined when active; smooth when healed | Irregular, spiculated, spiky edges (key red flag) |
| Cavitation walls | Thin to medium, smooth inner lining | Thick, irregular walls with uneven interior |
| Calcification | Common in old healed TB; dense, central | Rare; if present, usually eccentric (off-center) |
| Satellite nodules | Smaller nodules clustered around main lesion | Usually absent around primary tumor |
| Tree-in-bud (CT) | Strongly suggests active endobronchial TB | Not seen in primary lung cancers |
| Response on repeat scan | Active TB responds to ATT over weeks | Grows or stays the same regardless of ATT |
WHAT MOST BLOGS NEVER MENTION: The MRI Signal Test When CT alone cannot decide, MRI offers an additional layer of certainty. Research published in Frontiers in Oncology shows that TB lesions produce low signal intensity on T2-weighted MRI images, while lung cancer lesions show high signal intensity. The signal pattern in TB is also uneven, whereas cancer shows a more uniform signal. This distinction is particularly useful when dealing with mass-like TB that closely mimics a tumor on CT. Source: frontiersin.org/journals/oncology/articles/10.3389/fonc.2021.644150 |
Step 4: Blood Tests and Laboratory Markers
Imaging alone is never enough. Blood tests and laboratory markers add important diagnostic context. Here are the ones I rely on most frequently as a lung cancer specialist in Gurgaon:
• IGRA / Tuberculin Skin Test (TST): Positive results confirm TB exposure. But this does not confirm active disease and cannot rule out cancer. A positive IGRA means TB exposure, not TB diagnosis.
• Tumor Markers (CEA and CYFRA 21-1): Elevated carcinoembryonic antigen (CEA) and cytokeratin fragment 21-1 levels are valuable for distinguishing lung cancer from TB. Normal levels support TB; elevated levels raise cancer suspicion strongly. Source: Frontiers in Oncology 2021.
• ADA (Adenosine Deaminase): High ADA in pleural fluid typically points toward TB, though some cancers can also raise ADA, reducing its specificity alone.
• Gene Chip Detection: A newer rapid molecular test that identifies 17 types of Mycobacterium tuberculosis in 6-8 hours with a detection success rate approaching 100%. This is a significant advance for confirming or ruling out TB quickly. Source: Oncology Letters 2024.
• Sputum Smear and Culture: The traditional gold standard for TB. Effective when sputum is of good quality. However, sputum-negative TB is common, which means a negative test still cannot rule out TB definitively.
Step 5: PET-CT Scan for Metabolic Activity
When a CT scan leaves doubt, a PET-CT scan measures how much metabolic activity is happening inside a lesion. Cancer cells consume glucose at a much higher rate than TB granulomas. A high FDG uptake on PET-CT strongly suggests malignancy.
Research published in Molecular Imaging and Biology found that combined PET/CT with radiomics analysis achieves an AUC of 0.97 in separating active TB from solid lung cancer. That is near-perfect discrimination.
Step 6: Biopsy -- The Final Word
Imaging, blood tests, and clinical history can point strongly in one direction. But no diagnosis of lung cancer should be made or permanently excluded without tissue. Biopsy is the definitive step.
• Bronchoscopy with biopsy: Direct airway visualization with tissue sampling
• CT-guided biopsy: For peripheral lesions not reachable by bronchoscopy
• EBUS (Endobronchial Ultrasound): For mediastinal and hilar lymph nodes
• VATS (Video-Assisted Thoracoscopic Surgery): Minimally invasive biopsy and immediate resection if malignant, a procedure where thoracic surgeons with advanced training provide the best outcomes
WHAT MOST WEBSITES NEVER TELL YOU: Even Biopsies Can Be Misleading In some cases, biopsy samples taken from the wrong area of a mixed lesion may show granulomatous inflammation that looks like TB but surrounds an underlying tumor. Spindle-shaped cancer cells can resemble TB histology under a microscope. This is why multiple sampling points and experienced pathology review matter in ambiguous cases. Source: Frontiers in Oncology 2021 (frontiersin.org/journals/oncology/articles/10.3389/fonc.2021.644150) |
Concerned about a lung shadow that isn't responding to treatment? Dr. Parveen Yadav offers advanced lung cancer diagnosis including CT-guided biopsy, bronchoscopy, and VATS in Gurgaon. Consult a Lung Cancer Specialist Today →
What most patients and even some physicians do not realize is that tuberculosis and lung cancer are not just diagnostic lookalikes. TB is an actual risk factor for developing lung cancer later in life.
A cohort study cited in Infectious Agents and Cancer (Springer Nature) found that lung cancer incidence in TB patients was 269 per 100,000 people per year compared to just 153 per 100,000 in healthy controls, a 76% higher risk.
The mechanism appears to be chronic inflammation. Mycobacterium tuberculosis causes long-term inflammatory changes in lung tissue that damage DNA, suppress immune responses, and create conditions in which tumor cells can develop over years or decades.
Scar Carcinoma: When the Old TB Shadow Becomes a New Cancer
One of the most clinically important and underreported phenomena in chest medicine is scar carcinoma. Lung cancer, particularly adenocarcinoma, can grow within or adjacent to an area of old TB scarring.
This means a patient who was told their old TB shadow is "healed and stable" may actually be developing a new lung cancer within that same scar territory. When the X-ray is reviewed years later and the shadow looks "about the same," both the patient and the physician may conclude nothing has changed.
What to watch for: Any change in an old TB scar, even subtle growth, a new nodule appearing within the scarred area, or a new shadow near an old one, must be evaluated as a potential new malignancy and should not be assumed to be TB relapse.
The field of radiology is changing rapidly, and differential diagnosis between TB and lung cancer is one of the areas where artificial intelligence is making a real impact.
A December 2025 meta-analysis published in BMC Cancer analyzed 14 studies with 4,281 patients and found that CT radiomics models achieve a pooled AUC (accuracy) of 0.88 in distinguishing lung cancer from TB, significantly better than clinical models alone (AUC 0.77).
A 2025 study in European Radiology developed a 3D deep learning model trained on 1,160 patients across three hospitals that outperformed six radiologists in separating lung adenocarcinoma from tuberculoma.
AI-assisted diagnosis is not yet standard in most Indian hospitals. In the meantime, patients who receive ambiguous X-ray results should seek evaluation at specialized thoracic surgery centers where multidisciplinary diagnosis with CT, PET-CT, bronchoscopy, and biopsy is available under one coordinated team.
If you or a family member has been told there is a shadow on the chest X-ray, here is a clear, practical path forward:
• Do not panic. Most shadows are benign. But most shadows also require investigation before anyone can confirm that.
• Do not accept empirical ATT without a confirmed TB diagnosis. A shadow on X-ray is not sufficient grounds for starting six months of anti-TB treatment. Ask for a sputum test, IGRA, or CT scan first.
• Request a CT scan. A plain X-ray provides limited information. CT provides far greater detail about the size, shape, location, and behavior of the shadow.
• Ask about tumor markers. A simple blood test for CEA and CYFRA 21-1 can provide early guidance on whether cancer is possible.
• Seek a thoracic specialist if the shadow is large, irregular, or not responding to treatment. A shadow over 3cm, with irregular edges, or one that grows on follow-up imaging, needs specialist evaluation immediately.
• Get a second opinion for any ambiguous case. In medicine, ambiguity demands more information, not a faster guess.
At Chest Surgery India, led by Dr. Parveen Yadav, Director of Thoracic Surgery and Surgical Oncology at Artemis Hospital Gurgaon, patients receive comprehensive diagnostic evaluation including CT-guided biopsy, bronchoscopy, PET-CT interpretation, and minimally invasive surgery, all coordinated by a specialist team. If you are looking for lung cancer treatment in Gurgaon or need an expert oncologist in Gurgaon to review an ambiguous shadow, a free second opinion is available through the website.
• A chest X-ray shadow can represent tuberculosis, lung cancer, or several other conditions. It cannot be diagnosed by appearance alone.
• India's TB burden (25% of global cases) creates a high-risk environment for lung cancer misdiagnosis. Between 18% and 33.6% of lung cancer patients in India are initially given anti-TB treatment incorrectly.
• TB and lung cancer share symptoms but differ in lesion borders, cavity characteristics, satellite nodules, tree-in-bud CT patterns, and MRI signal intensity.
• Blood markers like CEA and CYFRA 21-1 are valuable early differentiators. The IGRA test confirms TB exposure but cannot rule out cancer.
• Old TB is a documented risk factor for lung cancer, raising incidence by 76% compared to healthy controls. Scar carcinoma is real and underreported.
• Tissue biopsy remains the only definitive confirmation of cancer. Even experienced radiologists and AI systems still require pathology as the final word.
• Never start anti-TB treatment for a chest shadow without confirmed microbiological or histological evidence of TB.
Rajan's story ended with surgery, chemotherapy, and a fight that was harder than it needed to be, simply because the diagnosis arrived too late. That outcome is not inevitable. The tools to get this right exist. The question is whether patients and physicians use them before assuming the shadow has an easy answer.
If you or someone in your family is living with an unexplained shadow on a chest X-ray, have you been offered a CT scan and a tissue diagnosis before starting any treatment? If not, that conversation needs to happen today.
If your chest X-ray report has left you with more questions than answers, don't wait. Call Artemis Hospital, Gurgaon at +91 9540210956 or visit Chest Surgery India to book your appointment →
Get a Free Second Opinion From Dr. Parveen Yadav Director, Thoracic Surgery and Surgical Oncology | Artemis Hospital, Gurgaon chestsurgeryindia.com/second-opinion-thoracic-surgeon-india.php Call: +91 9540210956 |
1. WHO Global Tuberculosis Report 2025 -- TB Incidence
2. JCO Global Oncology 2024: Spotlight on Lung Cancer Disparities in India
3. Lung India / PMC 2022: Clinical Profile of SCLC in North India
4. Indian Journal of Medical Research 2025: Lung Cancer Screening in India
5. The Lancet Regional Health Southeast Asia, July 2024: Lung Cancer Uniqueness in Southeast Asia
6. Oncology Letters 2024: Challenges in Differential Diagnosis of TB vs. Lung Cancer
7. Frontiers in Oncology 2021: Cancer or Tuberculosis -- A Comprehensive Review
8. BMC Cancer, Dec 2025: CT Radiomics Diagnostic Accuracy for LC vs TB
9. European Radiology 2025: Deep Learning Model for Lung Adenocarcinoma vs Tuberculoma
10. Molecular Imaging and Biology: PET/CT Radiomics for TB vs Lung Cancer
11. Infectious Agents and Cancer (Springer): TB as Risk Factor for Lung Cancer
12. National Cancer Registry Programme India: Cancer Incidence Estimates 2025
13. Indographics 2024: Imaging Spectrum in Pulmonary Tuberculosis
14. PMC: Pulmonary TB as Differential Diagnosis of Lung Cancer
15. University Hospitals Cleveland: How Common Are Lung Nodules?
16. Frontiers in AI, Feb 2025: AI Algorithm for TB Classification in CXRs
18+ Yrs Exp | 5,700+ Thoracic & Robotic Cancer Surgeries
Dr. Parveen Yadav is a Director and Senior Consultant in Thoracic and Surgical Oncology, specializing in minimally invasive and robotic lung and esophageal surgeries, with advanced training from AIIMS and Tata Memorial Hospital.
View Full Profile Esophageal Cancer Surgery Recovery Timeline: First Week to 3 Months
Esophageal Cancer Surgery Recovery Timeline: First Week to 3 Months
 Second Opinion for Esophageal Cancer in India: When and Why It Matters
Second Opinion for Esophageal Cancer in India: When and Why It Matters
 Robotic vs Open Esophagectomy: Which Surgery Is Better for Food Pipe Cancer?
Robotic vs Open Esophagectomy: Which Surgery Is Better for Food Pipe Cancer?
Understand the esophageal cancer surgery recovery timeline from the first week to 3 months, including diet, pain, walking, breathing exercises, follow-up, and warning signs.
Learn when to take a second opinion for esophageal cancer in India, what reports to share, and why expert review matters before surgery, chemotherapy, or radiation.
Compare robotic vs open esophagectomy for food pipe cancer. Learn differences in pain, recovery, blood loss, lymph node clearance, hospital stay, cost, and when open surgery may be better.
Copyright 2026 © Dr .Parveen Yadav all rights reserved.
Proudly Scaled by Public Media Solution!