


रमेश जी 47 साल के थे। दिल्ली-NCR में एक सरकारी दफ्तर में काम करते थे। एक रात नहाते वक्त उ
नकी पत्नी ने उनकी बाईं पसली के पास एक छोटी-सी उभरी हुई गाँठ महसूस की। रमेश जी को न कोई दर्द था, न कोई थकान। उन्होंने सोचा, 'बस चरबी होगी। तेल-मालिश से ठीक हो जाएगी।'
तीन महीने बाद वही गाँठ बड़ी हो गई थी। साँस लेते वक्त हल्की-सी खिंचन होने लगी। जब वो पहली बार मेरे OPD में आए, तो उनके चेहरे पर घबराहट थी। CT Scan और बायोप्सी रिपोर्ट ने बताया कि वो गाँठ एक malignant chest wall tumor था, जो पसली की हड्डी से निकल रहा था।
अगर वो तीन महीने पहले आ जाते, तो इलाज बहुत आसान होता।
यह कहानी सिर्फ रमेश जी की नहीं है। हर हफ्ते मेरी OPD में ऐसे कई मरीज़ आते हैं, जिन्होंने सीने की गाँठ को महीनों तक नज़रअंदाज़ किया, क्योंकि उन्हें पता ही नहीं था कि यह कब खतरनाक हो सकती है और कब नहीं।
इस ब्लॉग में मैं, Dr. Parveen Yadav, आपको वह सब बताऊंगा जो ज़्यादातर वेबसाइट्स बताना भूल जाती हैं: सीने में गाँठ के असली कारण, उसके खतरनाक लक्षण, जाँच का सफर, और उसका सही इलाज।
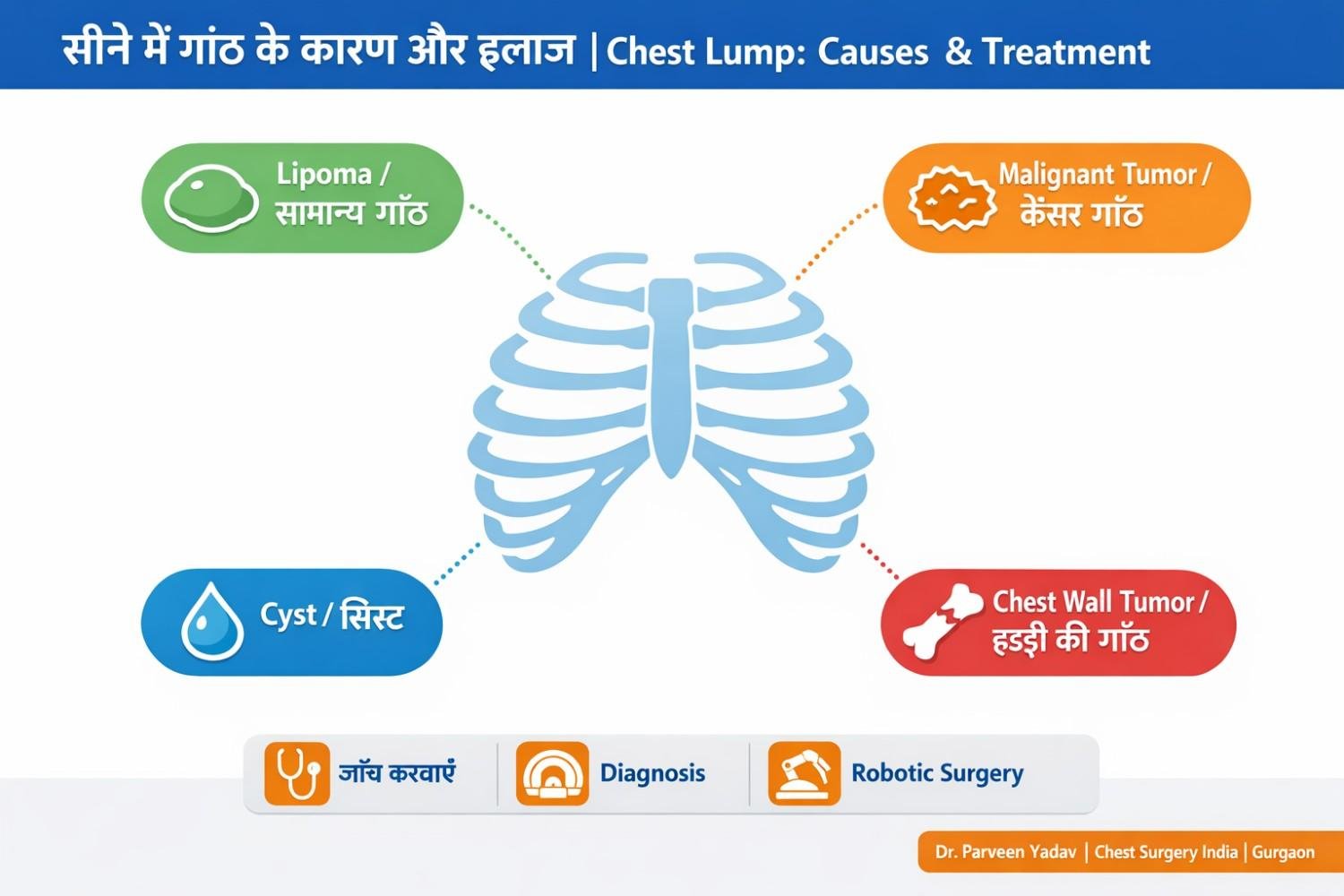
सीने में गाँठ (Chest Lump) का मतलब है छाती की दीवार पर, उसके अंदर या उसके नीचे किसी असामान्य उभार का होना। यह गाँठ त्वचा में, मांसपेशियों में, हड्डी में या कार्टिलेज में कहीं भी हो सकती है।
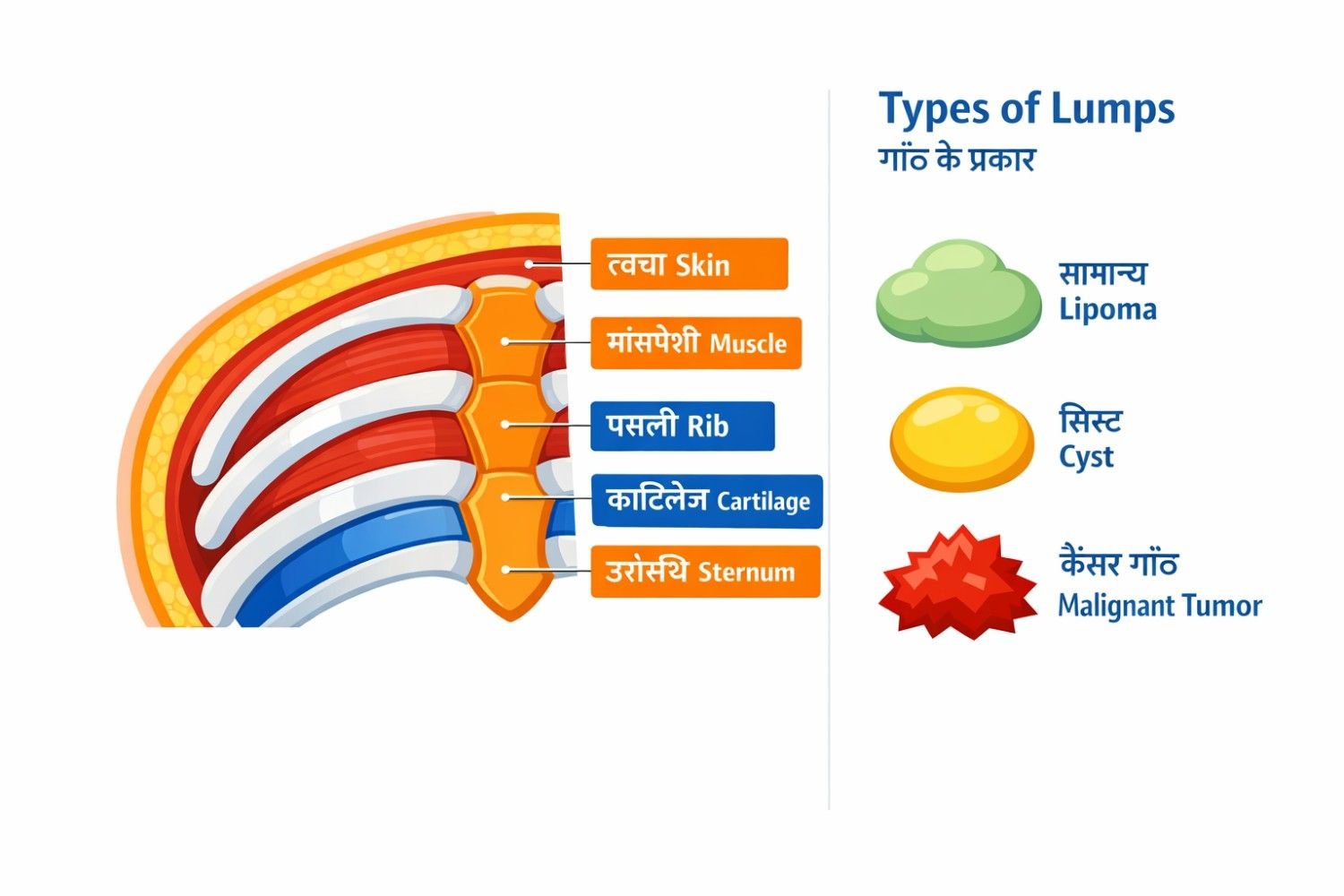
सीने की दीवार (Chest Wall) में यह परतें होती हैं:
• त्वचा (Skin) और चमड़े के नीचे की चरबी
• मांसपेशियां (Muscles)
• पसलियां (Ribs) और उनके बीच की मांसपेशियां
• कार्टिलेज (Cartilage) और उरोस्थि (Sternum)
दो मुख्य प्रकार की गाँठें होती हैं:
• Primary: जो सीधे chest wall की किसी परत से उत्पन्न होती है
• Secondary: जो किसी और अंग, जैसे फेफड़े या स्तन, के कैंसर से फैलकर यहाँ आती है
महत्वपूर्ण आँकड़ा: NCBI की 2024 की रिपोर्ट के अनुसार, primary chest wall tumors कुल आबादी के केवल 2% में होते हैं, और उनमें से लगभग 50% benign यानी गैर-कैंसर होते हैं। लेकिन बिना जाँच के यह तय करना असंभव है कि आपकी गाँठ किस श्रेणी में है।
ज़्यादातर लोग सोचते हैं कि chest lump हमेशा chest का ही cancer होता है। लेकिन असलियत यह है कि chest wall पर पाई जाने वाली बहुत सी गाँठें दूसरी जगह के cancer से फैलकर आती हैं, जैसे फेफड़े या स्तन का कैंसर।
1. Lipoma (चरबी की गाँठ): नरम, हिलने वाली, दर्दरहित गाँठ जो चरबी कोशिकाओं से बनती है। सबसे आम और लगभग हमेशा सुरक्षित।
2. Sebaceous Cyst: त्वचा के नीचे बनने वाली द्रव-भरी थैली। दबाने पर महसूस होती है।
3. Abscess (पस वाली गाँठ): बैक्टीरिया के कारण बनती है। बुखार, लालिमा और गर्माहट के साथ।
4. Hematoma: चोट के बाद खून जमा होने से बनी गाँठ।
5. Fibroadenoma: महिलाओं में हार्मोनल बदलाव के कारण, खासकर 14 से 35 साल में।
6. Gynecomastia: पुरुषों में निप्पल के पास, हार्मोन असंतुलन के कारण। यह cancer नहीं है लेकिन जाँच ज़रूरी है।
7. Osteochondroma: पसली या shoulder blade में हड्डी से निकलने वाली सबसे आम benign bone tumor।
8. Fibrous Dysplasia: हड्डी में normal bone की जगह रेशेदार ऊतक बन जाता है।
• Chondrosarcoma: chest wall का सबसे आम primary malignant tumor, जो कार्टिलेज से उत्पन्न होता है।
• Ewing's Sarcoma: बच्चों और युवाओं में पाया जाने वाला aggressive bone tumor।
• Lung Cancer का फैलाव: जब फेफड़े का कैंसर chest wall पर आ जाए।
• Breast Cancer का फैलाव (Secondary): chest wall पर metastasis।
• Lymphoma: lymph nodes की सूजन जो chest पर उभर सकती है।
सबसे ज़रूरी बात: अगर गाँठ sternum यानी सीने की बीच की हड्डी पर है, तो इसे हमेशा गंभीरता से लें।
Journal of Thoracic Disease (2024) के अनुसार sternal tumors लगभग हमेशा malignant होते हैं।
क्या आपने हाल ही में सीने पर कोई गाँठ महसूस की है? देरी न करें। अभी Chest Surgery India, Gurgaon में appointment बुक करें |
यह section अधिकांश websites पर नहीं मिलता। यह checklist आपको बताएगी कि अगले 48-72 घंटों में specialist से मिलना कितना ज़रूरी है:
• गाँठ 2 हफ्ते में बड़ी हो गई हो
• दबाने पर भी गाँठ न हिले, जड़ी हुई लगे
• बिना कारण बुखार, रात को पसीना, या वज़न घटना
• साँस लेने में तकलीफ या सीने में खिंचन
• खाँसी में खून आना
• गाँठ के ऊपर की त्वचा लाल, सख्त या धंसी हुई हो
• गाँठ sternum (सीने की बीच की हड्डी) पर हो
• पहले कभी कोई cancer रह चुका हो
• बांह या कंधे में अजीब दर्द के साथ गाँठ हो
अगर इनमें से कोई भी एक लक्षण है, तो यह सामान्य नहीं है। Thoracic Surgeon से मिलना ज़रूरी है।
यहाँ सबसे पूछे जाने वाले सवाल का जवाब है:
| विशेषता | सामान्य गाँठ | कैंसर गाँठ |
| दर्द | आमतौर पर नहीं | हो भी सकता है, न भी |
| बनावट | नरम, हिलने वाली | कठोर, जड़ी हुई |
| वृद्धि | धीमी या नहीं | तेज़, लगातार |
| त्वचा | सामान्य | लाल, सख्त, धंसी हुई |
| बुखार/थकान | नहीं | हो सकता है |
| साथ में लक्षण | कोई नहीं | खांसी, वज़न घटना |
याद रखें: दर्द नहीं है, इसका मतलब यह नहीं कि गाँठ safe है। Malignant tumors अक्सर महीनों तक painless रहते हैं।
यह section most websites पर नहीं मिलता। मरीज़ और उनके परिवार को अक्सर नहीं पता होता कि पहली visit में क्या expect करें:
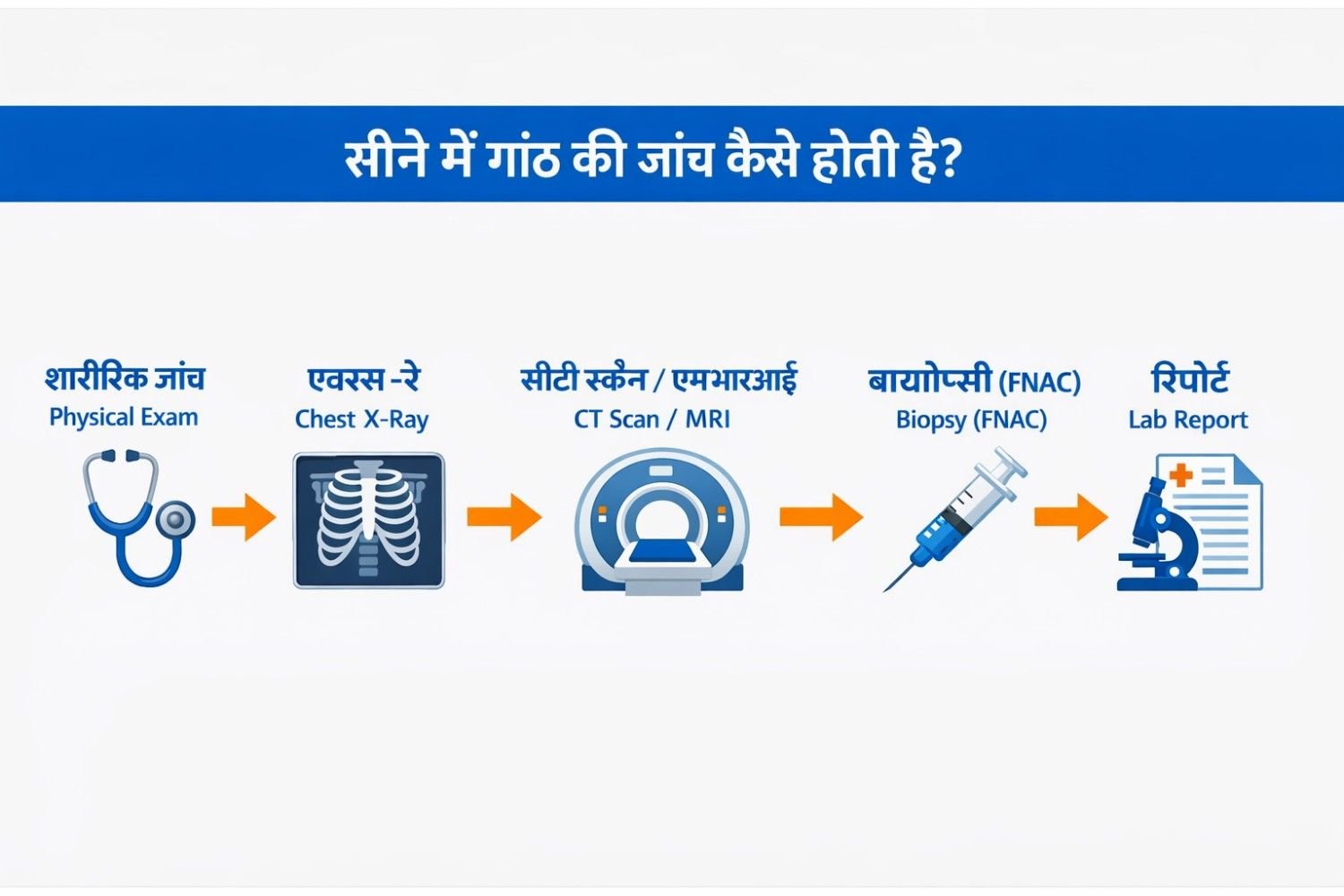
Step 1: Clinical Examination (शारीरिक जाँच)
डॉक्टर गाँठ का आकार, कठोरता, हिलना और आसपास की त्वचा की स्थिति देखते हैं। यह 5-10 मिनट की simple प्रक्रिया है।
• Chest X-Ray: पहला कदम। NCBI के अनुसार, 20% chest wall tumors यहीं detect हो जाते हैं।
CT Scan: हड्डी, मांसपेशी और blood vessels की जाँच के लिए सबसे अच्छा। (Source: NCBI, 2026)
• MRI: नरम ऊतकों की detailed जाँच के लिए CT से बेहतर।
• PET-CT: यह जानने के लिए कि cancer शरीर में और कहाँ फैला है।
• Ultrasound: सतह की गाँठ की guided biopsy के लिए उपयोगी।
Biopsy का मतलब है गाँठ से थोड़ा-सा tissue लेकर lab में जाँचना। यह cancer confirm करने का सबसे सटीक तरीका है।
• FNAC (Fine Needle Aspiration Cytology): पतली सुई से, बिना बेहोशी के, 10 मिनट में।
• Core Needle Biopsy: थोड़ी मोटी सुई, ज़्यादा accurate रिपोर्ट।
• Surgical Biopsy: जब needle biopsy काफी नहीं हो।
NCBI StatPearls (2025) के अनुसार, histopathologic evaluation (बायोप्सी की lab रिपोर्ट) diagnosis और treatment plan दोनों के लिए critical है। आज molecular genetic testing भी होती है जो treatment choice को और precise बनाती है।
• Watch and Wait: छोटी, stable, दर्दरहित गाँठ के लिए 3-6 महीने में follow-up।
• Aspiration: Cyst से सुई के ज़रिए द्रव निकालना।
• Surgical Removal: Lipoma, बड़े cyst या osteochondroma के लिए।
सर्जरी (Resection): कैंसर को जड़ से हटाना।
NCBI StatPearls (2025) के अनुसार, R0 margins (पूरी तरह साफ़ किनारे) के साथ surgical resection curative treatment की नींव है।
Chest Wall Reconstruction: पसली हटाने के बाद chest wall को titanium plates, mesh या muscle flap से दोबारा बनाना।
Chemotherapy: Surgery से पहले tumor छोटा करने के लिए, या बाद में।
Radiation Therapy: Surgery के बाद बची हुई कैंसर कोशिकाओं को खत्म करने के लिए।
Targeted Therapy / Immunotherapy: नए molecular treatments जो specific cancer cells को target करते हैं।
Chest Surgery India में उपलब्ध आधुनिक तकनीकें: • Da Vinci Robotic Surgery: छोटे चीरे, बेहतर precision, जल्दी recovery • VATS (Video-Assisted Thoracoscopic Surgery): बिना बड़े चीरे के chest wall तक पहुँच • 3D Imaging + PET-CT Fusion: tumor की exact location और spread • Chest Wall Reconstruction: titanium mesh, muscle flaps से structural repair |
Chest lump की जाँच करवाना चाहते हैं? Artemis Hospital, Sector 51, Gurgaon में Dr. Parveen Yadav की OPD में मिलें। Call: +91 9540210956 |
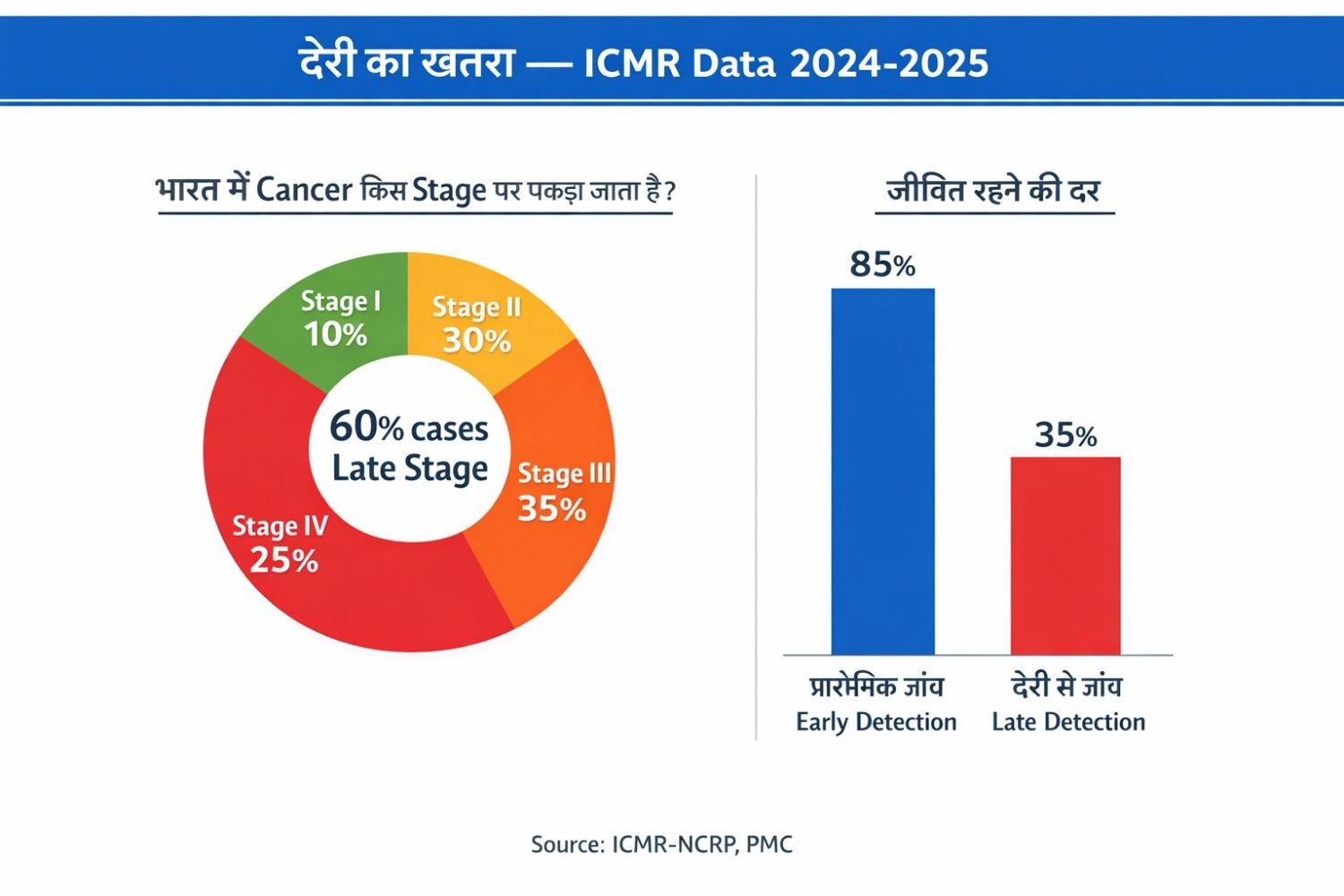
ICMR-NCRP की ताज़ा रिपोर्ट के अनुसार, India में cancer के कुल मामले 2022 में 14.6 लाख थे और 2025 तक यह 1.57 करोड़ तक बढ़ने का अनुमान है। India में हर 9 में से 1 व्यक्ति को जीवन में एक बार cancer होने का खतरा है।
सबसे चिंताजनक बात: PMC की study के अनुसार India में लगभग 60% breast और chest cancer के मामले Stage III या IV में diagnose होते हैं। मरीज़ तब तक नहीं आते जब तक गाँठ बहुत बड़ी न हो जाए।
देरी क्यों होती है? तीन सबसे बड़े कारण:
• 'अपने आप ठीक हो जाएगी' की सोच
• घरेलू नुस्खों पर भरोसा
• डॉक्टर के पास जाने में झिझक या डर
लेकिन यह सच है कि जितनी जल्दी diagnosis होती है, उतना ही बेहतर इलाज और उतनी ही लंबी ज़िंदगी। Chest wall के malignant tumors में average 5-year survival लगभग 60% है, जो early stage में बहुत बेहतर हो जाती है।
यह guidance ज़्यादातर Hindi websites पर नहीं मिलती:
1. शॉवर या नहाने के बाद, जब त्वचा ढीली हो, हाथ की उँगलियों से सीने पर धीरे-धीरे हाथ फेरें।
2. किसी भी उभार, कठोरता, या asymmetry को नोट करें।
3. गाँठ का अनुमानित आकार (किसी सिक्के से compare करें), hardness और movement नोट करें।
4. अगर 2 हफ्ते में बदलाव आए या कोई भी Red Flag symptom हो, तो doctor के पास जाएं।
Self-exam cancer का alternative नहीं है। यह सिर्फ early warning tool है।
रमेश जी की कहानी एक reminder है कि हमारा शरीर जब कोई संकेत देता है, तो उसे सुनना ज़रूरी है। सीने में गाँठ हमेशा cancer नहीं होती, लेकिन बिना जाँच के यह तय करना घातक हो सकता है।
इस ब्लॉग की मुख्य बातें: • 50% chest wall tumors benign होते हैं, लेकिन बिना जाँच के कोई नहीं जानता। • Sternum पर गाँठ, तेज़ growth, और कई लक्षण एक साथ आएं तो तुरंत जाँच करवाएं। • Chest X-Ray, CT, MRI और FNAC/Biopsy से accurate diagnosis होती है। • Early diagnosis में treatment बहुत आसान और ज़्यादा effective होता है। • India में 60% cases late stage में आते हैं, जो completely avoidable है। • Robotic और minimally invasive surgery से कम दर्द और तेज़ recovery होती है। |
एक सवाल सोचकर जाइए: अगर आपके किसी प्रियजन को ऐसी गाँठ हो, तो क्या आप उन्हें 3 महीने इंतज़ार करने देंगे?
अगर जवाब 'नहीं' है, तो खुद के लिए भी यही करें।
Free Second Opinion लें: सीने की गाँठ के बारे में अभी पूछें Second Opinion Thoracic Surgeon India | Call: +91 9540210956 | Artemis Hospital, Gurgaon |
नहीं। NCBI के अनुसार, लगभग 50% primary chest wall tumors benign होते हैं। Lipoma, cyst और fibroadenoma बहुत आम और सुरक्षित हैं। लेकिन बिना जाँच के यह तय करना संभव नहीं है।
नहीं। FNAC एक बहुत पतली सुई से की जाती है, जो 5-10 मिनट में हो जाती है। अधिकांश मरीज़ इसे injection जैसा बताते हैं।
Thoracic Surgeon या Surgical Oncologist से। अगर Gurgaon या Delhi-NCR में हैं, तो chest wall specialist ज़रूरी है क्योंकि diagnosis और treatment दोनों ही specialized होते हैं।
यह गाँठ के प्रकार पर निर्भर करता है। Cysts को aspiration से, infections को antibiotics से ठीक किया जा सकता है। लेकिन solid tumors (benign या malignant) को अक्सर surgical removal की ज़रूरत होती है।
हाँ। Robotic और minimally invasive surgery से कम blood loss, छोटे चीरे और तेज़ recovery होती है। Gurgaon के Artemis Hospital में Da Vinci Robotic System available है।
Sternum (सीने की बीच की हड्डी) पर गाँठ को हमेशा गंभीरता से लें। Research बताती है कि sternal tumors अक्सर malignant होते हैं। तुरंत Thoracic Surgeon से मिलें।
निम्नलिखित विश्वसनीय medical sources से डेटा लिया गया है:
1. NCBI StatPearls: Chest Wall Tumors (2025-2026)
2. ICMR-NCRP: Cancer Incidence Estimates India 2022 & Projection 2025 (PMC)
3. PMC: Benign Tumors of the Chest Wall, Journal of Thoracic Disease (2024)
4. PMC: Chest Wall Tumors and Surgical Techniques (2022)
5. AIIMS New Delhi: Malignant Chest Wall Tumors, Ann Surg Oncol (2024)
6. PMC: Breast Cancer in India: Present Scenario and Challenges
7. NCBI: Lung Cancer Screening in India (PMC, 2024)
18+ Yrs Exp | 5,700+ Thoracic & Robotic Cancer Surgeries
Dr. Parveen Yadav is a Director and Senior Consultant in Thoracic and Surgical Oncology, specializing in minimally invasive and robotic lung and esophageal surgeries, with advanced training from AIIMS and Tata Memorial Hospital.
View Full Profile
छाती के X-Ray में सफेद धब्बा दिखने का मतलब हमेशा कैंसर नहीं होता। जानें इसके संभावित कारण, टीबी और लंग कैंसर में अंतर तथा जरूरी जांच।
Found a lung nodule on your CT scan? Learn how lung nodules differ from lung cancer, which features raise concern, and when biopsy or surgery may be required.

Understand the esophageal cancer surgery recovery timeline from the first week to 3 months, including diet, pain, walking, breathing exercises, follow-up, and warning signs.
Copyright 2026 © Dr .Parveen Yadav all rights reserved.
Proudly Scaled by Public Media Solution!